When discussing potentially harmful pests, a common one you’ll often hear about is ticks. These strange creatures latch onto a host through physical contact. You might be out enjoying nature and inadvertently come in contact with them in the grass or by brushing against one on a tree branch. These opportunistic pests can also be transferred onto you by another person or your pet.
Unfortunately, these pests can negatively impact your health. While mosquitoes are known to carry certain diseases like West Nile or Zika, infected ticks can transmit Lyme disease, which can cause serious health issues for many people. The thought of ticks may have you asking the question: Where did Lyme disease originate? To help you better understand Lyme disease and its origin, the pest control experts at Mosquito Joe® have some valuable information to share.
What Is Lyme Disease?
Lyme disease is a product of the bacterium Borrelia burgdorferi, commonly found in ticks in the United States. While you can get Lyme disease from a tick bite, not all ticks carry the disease. But you should take extra precautions, especially when walking in areas that are heavily wooded or have a lot of tall grass.
Symptoms of Lyme Disease
Symptoms of Lyme disease can vary between individuals who are infected, and symptoms don’t always show up immediately. Lyme disease skin manifestations and other symptoms can begin to appear anywhere from 3 days to a month after the initial bite.
If you have be bitten by a tick or suspect you have Lyme disease, here are some critical signs to look for:
Stage One
A standard bug bite: Most people won’t know they’ve received a bite from a tick because they won’t feel the initial bite. Tick saliva has a chemical that acts as a local anesthetic. The chemical numbs the bite area, which often results in a bite going undetected. However, things can change by day three.
Rash: Rashes are common Lyme disease skin manifestations. They may not hurt, but they’ll be warm to the touch. It’s best to stay away from scratching it. The tell-tale sign of a tick bite is a bulls-eye rash that appears around the bite area. The rash is red in the center and has additional red rings of red around it, which may increase in size over time.
Fever, headache, chills: In addition to a rash, you may also experience a high fever, headache, and/or chills.
If you experience any of these symptoms after a tick bite, it’s important to seek medical attention as soon a s possible.
Stage Two
Failing to treat stage one of Lyme disease can lead to more severe symptoms in stage two, such as:
Widespread rashes over your entire body.
Extreme muscle soreness and weakness.
Facial weakness on one or both sides of the face.
Pain in lower limbs.
Once again, if any of these symptoms appear, you should seek help from a medical professional.
Stage Three
Stage three of Lyme disease includes many of the symptoms in stage two. However, a person may experience more pain and swelling in localized areas, such as the knees and other joints. You may also experience arthritis in certain joints.
FAQs About Lyme Disease
How Is Lyme Disease Diagnosed?
Lyme disease is tricky to diagnose because it shares similar symptoms with many other medical conditions. However, if you have been bitten by a tick or suspect that you may have Lyme disease, a blood test should be taken to confirm any presence of the disease.
It’s important to note that depending on when the test is administered, blood tests for Lyme disease are not always 100% accurate. During the early stages of the disease, a blood test may come back negative. However, if you receive positive results from your first blood test, you’ll be asked to submit another to determine the severity of your Lyme disease.
How Is Lyme Disease Treated?
Additional research still needs to be done to improve Lyme disease treatments. It is currently treated with antibiotics While this treatment is effective in the early stages, many people report experiencing long-term effects like fatigue and muscle pain.
Can You Get Lyme Disease From Mosquitoes?
When you hear that one pest has a disease, it’s not far-fetched to think others may carry the same disease. While mosquitoes can carry insect-borne illnesses, according to the CDC (Center for Disease Control), the answer is no.
There’s currently no evidence that indicates you can get Lyme disease from mosquitoes. Additionally, mosquito bites are typically very brief, whereas ticks must hang onto their host for hours or days to fully transmit Lyme bacteria.
Long-Term Complications of Lyme Disease
As mentioned above, if you don’t address the symptoms of Lyme disease during the initial stages, it can lead to longer-term complications. Even after treatment, some people still experience side effects of the disease, such as:
Bodily aches
Arthritis in knees and other joints that don’t seem to go away
Lethargy
You could also face some neurological effects of Lyme disease that can impact your memory, facial muscles, and the muscles around your neck.
Lyme disease can be very debilitating for those infected, but this doesn’t mean you should never venture outside again. There are steps and precautions you can take to mitigate the risks. Follow these simple steps when visiting heavily wooded or sparsely populated areas, especially areas with tall, unkempt grass:
Use tick repellants: Spray tick repellant on your clothes and shoes before going to a grassy or wooded area. It’ll keep them away while you’re outdoors.
Wear light-colored clothing: Ticks and other pests are attracted to dark colors. Wear lighter colors to reduce the risks and to help someone spot one on you.
Dress for protection: Although it might be warm during the summer, you’ll still need to wear the proper clothing when venturing outdoors. Avoid wearing open-toed shoes in areas where ticks may lurk. Also, wear long-sleeved shirts and/or pants for the time you’re outside to avoid a tick latching onto your legs.
Hire service professionals: Rather than waiting to find out if you have ticks on your property, be proactive and hire a professional service. A barrier spray treatment provides a protective shield around your property, keeping pests out and away from your family and pets.
Check for ticks: Always check for ticks if you’ve been engaging in an outdoor activity. Have someone inspect your clothing or use a mirror to check yourself and areas you cannot easily see.
Protect Yourself From Ticks and Other Annoying Pests
Insects are innovative, adaptable creatures, which explains why they have been in existence for so long. Protecting you, your family, and pets from the dangers of ticks requires a proactive approach. If you enjoy the outdoors, take preventive measures to keep ticks and other pests off your property.
For ultimate peace of mind, call on the professionals at Mosquito Joe®. Our tick control services are developed to protect your property from potentially harmful insects. We offer a range of pest control services. that are all backed by the Neighborly Done Right Promise™, which ensures your satisfaction. You don’t have to spend all your time indoors, because Mosquito Joe is making the outdoor fun again! Request a free quote today!
The symptoms of those suffering from Lyme disease are different but the cause of the illness is the same: infected ticks. These celebrities give visibility to Lyme disease and advocate for treatment and a cure.
While it’s important to be mindful of ticks when camping and hiking, they can also be found in parks, walking trails, and even our own backyards. Tick prevention can start at home by eliminating places where ticks like to hide. Keep your yard mowed and trees trimmed. If you are in an area where ticks are active, make sure to wear long sleeves and pants and apply a tick repellent with DEET or Permethrin.
Mosquito Joe knows what a pest ticks can be, that’s why we offer tick control as one of our signature services. We target bushes and shrubbery, which helps keep ticks out of your yard and creates a barrier around your property, protecting you against the risk of tick-borne illnesses. Call us today at or request a free quote on our website.
To learn more about Lyme Disease or other illnesses that are caused by outdoor pests, visit our learning center.
Lyme disease is one condition that doesn’t care whether or not you’re a celebrity or a normal person. In fact, there are a plethora of stars who have spoken out about their own lifelong struggles with the condition. There are over 30,000 cases of the tick-borne illness reported each year. Among those are celebrities we frequently see on TV or on magazine covers; others are sports icons and some are Grammy award winners.
You’re hiking in the woods. Suddenly, you feel something extremely itchy. You scratch it, and find a rash like a red bull’s eye on your body. Looking closely, you see a small hole. And it’s painful. If you don’t act quickly, your life could be in danger. What to do if you find a tick on you? How long does a tick need to be on you? How do you remove a tick that is embedded?
Note: This video is not intended to be a substitute for professional advice, diagnosis, or treatment. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have seen on this channel. If you think you may have an emergency, call your doctor, the ambulance or the police immediately. Underknown does not recommend or endorse any specific tests, physicians, products, procedures, opinions, or other information that may be mentioned in this video. Reliance on any information provided by Underknown is solely at your own risk.
The country singer opened up about her struggle with Lyme disease in July 2018, stating she suffered from dysphonia which affected her vocal cords. The disease kept her from touring and even singing. “I never thought I would sing again,” Twain said. Thanks to physical therapy and vocal training, Twain has released a new album and resumed touring. Shania Twain – Giddy Up! – Lyrics (youtube.com)
Twain’s symptoms were quite alarming: dizziness, balance issues, and even millisecond blackouts while performing on stage. It took several years for doctors to connect her voice problems to Lyme disease. The infection caused nerve damage that affected her vocal cords, resulting in a condition called dysphonia. Although her voice was permanently impacted, she feels fortunate that the disease didn’t attack another part of her body, like her heart. Despite the challenges, Twain now owns her different voice and continues to inspire fans worldwide23.
The result was numerous bouts of severe Lyme disease symptoms.
Because of his struggle, Baldwin is vigilant in checking his children for ticks after they’ve been outdoors. “I want my kids to grow up riding horses and bikes and enjoying themselves every day and not have to spend every day with us going over them with a magnifying glass to make sure they don’t have any ticks on their body or their dogs, but that is part of the lifestyle of where I live,” he said. Since then, Baldwin has been cautious about letting his six children play outdoors in the Hamptons, an area known for ticks. He and his wife, Hilaria, are vigilant about tick prevention, especially during mild winters when ticks become more active1.
Pop sensation, Justin Bieber, announced his battle with Lyme disease in January 2020. “It’s been a rough couple years but getting the right treatment that will help treat this so far incurable disease and I will be back and better than ever,” Bieber said. The singer plans to use his voice to create content on YouTube about chronic illness.
Members of the Hadid Family
Yolanda Hadid, of The Real Housewives of Beverly Hills fame, has been vocal about her battle with Lyme disease. Yolanda has published a book chronicling her experience living with the illness entitled “Believe Me: My Battle with the Invisible Disability of Lyme Disease.” Recently, the former model admitted after nearly a year of remission, her symptoms have returned. At the Global Lyme Alliance, Yolanda said she realizes “the higher purpose of [her] journey is to continue to bring awareness to this awful disease until the change is made.” Her children, Bella and Anwar Hadid, also have the chronic illness.
In a letter to fans, Lavigne revealed she had been fighting Lyme disease. The singer started The Avril Lavigne Foundation in 2010 to support causes such as Race to Erase MS, Special Olympics, and UNICEF, in addition to Lyme disease. In October 2018, Lavigne joined the Board of Directors for the Global Lyme Alliance. Her most recent album, “Head Above Water,” addresses her battle with the chronic disease. “This is me and my fight. This album tells my story,” Lavigne said.
Kris Kristofferson
Kristofferson’s doctors originally told him his deteriorating memory was due to Alzheimer’s disease. After many years of strenuous testing, it was clear the singer had been misdiagnosed; after a positive test for Lyme disease, his symptoms were correctly identified. With the proper treatment, Kristofferson’s condition improved. A friend said of the iconic artist, “Kris is as sharp as he’s been in the past 20 years because of his treatments.”
The progress of science in the last 400 years is mind blowing.
Who would have thought we’d be able to trace the history of our universe to its origins 14 billion years ago? Science has increased the length and the quality of our lives, and the technology that is commonplace in the modern world would have seemed like magic to our ancestors.
For all of these reasons and more, science is rightly celebrated and revered. However, a healthy pro-science attitude is not the same thing as “scientism,” which is the view that the scientific method is the only way to establish truth. As the problem of consciousness is revealing, there may be a limit to what we can learn through science alone.
Perhaps the most worked out form of scientism was the early 20th-century movement known as logical positivism. The logical positivists signed up to the “verification principle,” according to which a sentence whose truth can’t be tested through observation and experiments was either logically trivial or meaningless gibberish. With this weapon, they hoped to dismiss all metaphysical questions as not merely false but nonsense.
These days, logical positivism is almostuniversally rejectedby philosophers. For one thing, logical positivism is self-defeating, as the verification principle itself cannot be scientifically tested, and so can be true only if it’s meaningless. Indeed, something like this problem haunts all unqualified forms of scientism. There is no scientific experiment we could do to prove that scientism is true; and hence if scientism is true, then its truth cannot be established.
In spite of all of these deep problems, much of society assumes scientism to be true. Most people in the UK are totally unaware that “metaphysics” goes on in almost every philosophy department in the country. By metaphysics, philosophers don’t mean anything spooky or supernatural; this is just the technical term for philosophical, as opposed to scientific, inquiry into the nature of reality.
Truth without science
How is it possible to find out about reality without doing science? The distinguishing feature of philosophical theories is that they are “empirically equivalent,” which means you can’t decide between them with an experiment.
Take the example of my area of research: the philosophy of consciousness. Some philosophers think that consciousness emerges from physical processes in the brain—this is the “physicalist” position. Others think it’s the other way around: consciousness is primary, and the physical world emerges from consciousness.
A version of this is the “panpsychist“ view that consciousness goes all the way down to the fundamental building blocks of reality, with the word deriving from the two Greek words pan (all) and psyche (soul or mind).
Still others think that both consciousness and the physical world are fundamental but radically different—this is the view of the “dualist.” Crucially, you can’t distinguish between these views with an experiment, because, for any scientific data, each of the views will interpret that data in their own terms.
For example, suppose we discover scientifically that a certain form of brain activity is correlated with the conscious experience of an organism.
The physicalist will interpret this as the form of organization which turns non-conscious physical processes—such as electrical signals between brain cells—into conscious experience, whereas the panpsychist will interpret it as the form of organization which unifies individual conscious particles into one larger conscious system. Thus we find two very different philosophical interpretations of the same scientific data.
If we can’t work out which view is right with an experiment, how can we choose between them? In fact, the selection process is not so dissimilar from what we find in science. As well as appealing to experimental data, scientists also appeal to the theoretical virtues of a theory, for example how simple, elegant and unified it is.
Philosophers too can appeal to theoretical virtues in justifying their favored position. For example, considerations of simplicity seems to count against the dualist theory of consciousness, which is less simple than its rivals in so far as it posits two kinds of fundamental stuff—physical stuff and consciousness—whereas physicalism and panpsychism are equally simple in positing just one kind of fundamental stuff (either physical stuff or consciousness).
It could also be that some theories are incoherent, but in subtle ways that require careful analysis to uncover. For example, I have argued that physicalist views of consciousness are incoherent (although—like much in philosophy—this is controversial).
There is no guarantee that these methods will yield a clear winner. It could be that on certain philosophical issues, there are multiple, coherent, and equally simple rival theories, in which case we should be agnostic about which is correct. This would in itself be a significant philosophical finding concerning the limits of human knowledge.
Philosophy can be frustrating because there is so much disagreement. However, this is also true in many areas of science, such as history or economics. And there are some questions on which there is a modest consensus, for example, on the topic of free will.
A tendency to mix up philosophy with a growing anti-science movement undermines the united front against the real and harmful opposition to science we find in climate change denial and anti-vax conspiracies.
Like it or not, we can’t avoid philosophy.
When we try to do so, all that happens is we end up with bad philosophy. The first line of Stephen Hawking and Leonard Mlodinow’s book “The Grand Design” boldly declared: “Philosophy is dead.” The book then went on to indulge in some incredibly crude philosophical discussions of free will and objectivity.
If I wrote a book making controversial pronouncements on particle physics, it’d be rightly ridiculed, as I haven’t been trained in the relevant skills, haven’t read the literature, and haven’t had my views in this area subject to peer scrutiny. And yet there are many examples of scientists lacking any philosophical training publishing very poor books on philosophical topics without it impacting their credibility.
This might sound bitter. But I genuinely believe society would be deeply enriched by becoming more informed about philosophy. I have hope that we will one day move on from this “scientistic” period of history, and understand the crucial role both science and philosophy have to play in the noble project of finding out what reality is like.
One of the most difficult problems in neuroscience and philosophy is the study of consciousness. How does consciousness arise from physical matter?
In a 1995paper, philosopher David Chalmers dubbed this question “the hard problem.” The “easy” problem, he said, is figuring out how the brain does things like see, learn, think and make decisions.
While not exactly easy, at least these questions can be approached scientifically and, given the right techniques and technology, might eventually be solved. The “hard” problem, according to Chalmers, is figuring out why and how, when we see, learn, think and so on, we have a subjective experience.
Some experts think we’re getting close to solving that problem. Others think it might never be solved.
Katrina Krasich is a neuroscientist at Elon University and a two-time winner of the Neurophilosophy of Free Will World Wide Competition. Krasich says there has been considerable progress in recent years on the “easy” problem.
“We’ve been at least able to assess what I will call enabling conditions,” she says, “what allows consciousness to emerge, or at the very least, what conditions prevent consciousness from occurring.” Much of this progress, Krasich says, is due to better technologies for studying the brain in action.
That still doesn’t tell us how we get from meat to mind, but many people in many different fields of study — neuroscience, philosophy, information science, mathematics, linguistics, psychology, physics and more — are working on it.
One of the most promising current theories of consciousness isintegrated information theory (IIT), developed by Giulio Tononi, a neuroscientist at the University of Wisconsin. Consciousness, according to IIT, requires the integration of a huge amount of information.
Consciousness emerges in a system — in any system — when that information is sufficiently integrated. It’s not enough for a system to possess loads of information (as does your phone); it has to connect all that information meaningfully. And the more that information is integrated, the more conscious the being that integrates it.
IIT has received a lot of criticism because it allows for the possibility of consciousness, or at least a very rudimentary form of consciousness, in places we normally wouldn’t expect to find it — in a proton, for example. It’s somewhat like a neuroscientific version ofpanpsychism, the idea that consciousness is inherent in all matter.
Global Workspace Theory
A competing theory is known asGlobal Workspace Theory (GWT), first developed in the 1980s by Bernard Baars. GWT holds that consciousness is formed in an internal “workspace” as the brain processes information. According to GWT, consciousness is a byproduct of the information processing that underlies behavior.
Others are studying the workings of the brain using modern technologies, such as functional magnetic resonance imaging (fMRI) and transcranial magnetic stimulation, in attempts to unravel the conundrum of consciousness. Some, includingChalmers, now co-director of NYU’s Center for Mind, Brain and Consciousness, are even probing theconnection between consciousness and quantum mechanics.
While attending the annual meeting of the Association for the Scientific Study of Consciousness (ASSC) in Bremen, Germany, in 1998, Chalmers and Christof Koch, a neuroscientist and champion of IIT, went out for drinks one evening and got to talking about the future of consciousness science.
Koch bet his friend a case of wine that within 25 years, science would have found clear (note the word ‘clear’) neural correlates of consciousness. Koch now insists he was genuinely convinced that science would meet that deadline, even if some of that conviction was due to youthful exuberance.
This June, at the 2023 conference of the ASSC — 25 years after the wager — the bet was settled. Experiments using fMRI and implanted brain electrodes looked at the brain patterns of human patients, and compared those to the conscious experience the patients reported when looking at pictures of faces and other objects. The results — presented at the conference — seemed to support some of the predictions of both GWT and IIT. However, the results were anything but clear.
Koch admitted that these results showed that no clear neural correlates had been found.
He graciously presented his friend with six bottles of 1978 Madeira. (Chalmers says he was delighted — he’d expected a 1998 vintage.) Koch also asked for a rematch, double or nothing. Within another 25 years, Koch wagered, clear evidence would be found. Chalmers didn’t hesitate to take the bet but says he’ll be happy if he loses this time and thinks that the chances he will lose are better now, owing to improved technologies for observing the brain.
However, neither of the wagers requires solving the hard problem. Nailing down the neural correlates of consciousness, even if it can be done, won’t necessarily show how consciousness emerges from matter. That question has philosophical implications that may or may not be amenable to science.
A New Generation of Consciousness
In 25 years, Chalmers will be 82 and Koch 92. Krasich, who is far younger than both men, is part of a new generation of scientists working on this problem. She describes herself as having a “bright-eyed and bushy-tailed approach,” perhaps not confident that the problem will be solved but hopeful. She expects that continued development of technology and more scientific discovery will lead to progress. “But,” she adds, “it’s really unclear if we’ll be able to answer with certainty how consciousness emerges.”
She is confident of one thing, though. Any progress will be the result of an interdisciplinary approach. “I don’t think that my field of study will have the answer. I don’t think that computer science will have the answer. I think that it will be an interdisciplinary answer.” There may well be more wagers to come as teams of scholars continue to tackle the perplexing problems of consciousness, both “hard” and “easy.”
My story is a testament that love is everything, prayers are answered, and miracles do happen. Christy’s resilience and determination are truly inspiring.
Despite her ongoing battle with lung cancer, she continues to embrace life with courage and zest. Her story reminds us all to cherish each moment and find joy even in the face of adversity.
In 2006, I didn’t feel well. I was really tired, had shortness of breath, chest pain, back pain, a constant, wheezing cough. I would later discover these are five symptoms of lung cancer. I always did small things to stay in shape, but after walking up a flight of stairs and not being able to breathe, I decided it was time to go to the doctor.
My primary care physician checked my heart, my spine and tested me for asthma. She said everything looked normal, to take Prilosec for 30 days, and schedule a follow-up visit. That was on a Tuesday. That Friday, I received a call that the X-ray technician had found several spots on my lungs.
At the time, I was only 38. I’d never smoked a day in my life, I’d been a lifetime athlete, attending college on a basketball and track scholarship, and we didn’t have any cancer history in my family.
In September 2006, after three months of testing in five different hospitals, I received a call from my doctor that he wanted me to come in to go over my test results. So, my husband Rich, my family and I met at the doctor’s office. The doctor shared that he and his team reviewed the results and that it was stage IV lung cancer. Everyone in the room began to cry.
By the time I was diagnosed, the cancer had spread to both of my lungs, my neck and I had a tumor the size of a golf ball in my chest. As the doctors shared the news, they explained I only had a 2% chance of living and that most with my diagnosis die within the first year. They were basically telling me I was going to die.
I never believed I would die. To me, thinking that way would be a waste of time. I heard the 2% living, not the 98% dying. So, when I got the news that day, I didn’t cry and I didn’t ask “why me?” I couldn’t go back in time and change anything, so why dwell on it? I set my sights on where I wanted to be and decided to spend my time living my life. All I could do was control the future and what I was going to do next. I knew it was time for me to put on my game face and that is exactly what I did! I looked at my diagnosis as a challenge or a competition that I was going to win. There was no way I was going to allow cancer to beat me.
At that point, my only chance of surviving was with chemotherapy because the cancer had spread throughout my body. About a month later it was time for me to start chemo. I was full of energy and determination, but the thought of putting poison in my body was something I needed to deal with.
So, I dealt with it my way. I went to the ladies’ restroom, locked the door, got down on my knees and prayed for God to take care of me and give me the strength I needed.
I immediately felt the urge to dance, so I did. I stood at the ladies’ room mirror and sang really loud and danced really hard. It was what I needed; I was then ready to start chemotherapy.
Every other week for 17 months, I’d show up for chemo.
They’d stick a needle in the top of my hand, and I would sit there for an hour and a half while they pumped my body with medicine that I knew was going to make me feel awful. And every day afterward, I would get up and go to work. No way was I going to let the cancer win.
I took control of the situation. I didn’t let cancer define me. My hair fell out, so I wore cute baseball hats. I gained 20 pounds, so I bought new clothes. I made sure my personal calendar came first, and my medical calendar came second.
We bought a motorcycle, we went on a hot air balloon, we went parasailing, and we traveled to so many places. Also, during this time my niece Keagan Christy aka Little C came into the world. I continued to live my life to the fullest despite my situation. After nearly a year and a half of chemotherapy, I was cancer free for the first time.
In 2013, the cancer returned. During a routine checkup, they found a tumor the size of a walnut in my chest. In June of 2013, they opened my chest and breastbone and removed my thymus and pericardium, a procedure that was almost unheard of for a stage IV lung cancer patient. I now have a seven-inch scar on my chest from the incision. I’m not ashamed of my scar and I don’t try to hide it. After six weeks of recovery from my surgery, I was cancer free for the second time.
I had always wanted to run a half marathon.
After winning against stage IV lung cancer twice, I decided to go after that goal. Six months after my open chest surgery I began training and in April 2014, I ran my first half marathon in 2 hours and 26 minutes. But just a week later, at my routine checkup, I found out I had stage IV lung cancer for the third time.
In May of 2014, the doctors determined I had several tumors in the lining of my lungs.
I went after round 3 just like I did with rounds 1 and 2—with drive and determination. And, as you might have guessed, I danced! And I did all the other things I loved to do.
I went to the World Series and a Fleetwood Mac Concert. I traveled to Key West, New Orleans and Costa Rica. I took my dad to an Indiana Colts football game and got to be a Coin Toss Captain at a Chiefs football game. I didn’t allow cancer to control my life, instead I was in control.
A year and 17 rounds of chemo later, the doctors decided to take me off the chemo to monitor me. In February 2017, I received fabulous news that I was cancer free for the third time.
But in October 2017, the doctors discovered two spots on my lungs.
After a needle biopsy, I was diagnosed with stage IV lung cancer for the fourth time. The good news is that although the cancer is active, it is stable and there are no signs of new disease, so no treatment is needed at this time.
As always, I’m facing round 4 by continuing to live my life to the fullest. We went to Aruba and the Virgin Islands. We saw Hank Williams Jr. and Bob Seger in concert. I took my niece to see Ariana Grande in concert. I took my dad on a helicopter ride.
We moved to the Lake of the Ozarks where every day I get to wake up to a beautiful sunrise, watch eagles fly, listen to the birds sings, and look up and see a million stars in the night sky.
I ran the Lake of the Ozarks 10K. As I approached the third mile, I looked over at the incredible water and then up at the sky and thanked God for the wonder of it all.
When Rich and I met over 28 years ago on the dance floor at a sports bar, he had no idea that his wife would be faced with the deadliest form of cancer. I’ve always wished better for him. He didn’t sign up for this. But God knew our plans and that’s why he put us together. I wouldn’t be here today without Rich. I’m so very blessed that he’s mine.
My dad doesn’t like talking about me having cancer, but he did eventually share one story with me. He said that the day I called and told them I had cancer, he got in his truck and turned on the radio. The first song he heard was “Live Like You Were Dying” by Tim McGraw, which is a perfect example of what this is like. But I don’t live like I’m dying.
I live like I’m alive.
A friend of mine describes my story as my “Victory March” and I like that. Throughout my “Victory March” I have leaned on what I learned from my parents and from my coaches.
I continue to listen to my inner voice saying, “You can do it,” “Don’t give up” and “I’m strong.”
If I had one wish, it would be for everyone to experience what I have. Not the cancer, but the power of love, prayer and the desire to live life to the fullest. If I hadn’t been diagnosed with cancer, I would never have experienced and felt the love, support, and friendship that has been given to me from so many people.
I don’t spend any time thinking about the fact that I have cancer. Instead I focus on being happy and alive! I feel truly blessed. I know that God has chosen me to provide hope and strength to others that will be diagnosed with this disease.
Cancer will be part of my life for the rest of my life.
I’m proud of that. I have had the privilege of participating in countless research trials.
I always say yes! This research could potentially save lives by providing better medicines and treatments for future patients.
I have also raised over three million dollars to support defeating lung cancer. To me, that’s what it’s all about—being happy and making a positive difference. On September 26, 2019, l celebrated being a 13-year stage IV lung cancer survivor. My doctors call me a miracle. That day, I opened the windows and sunroof of my car and drove down the highway with the sun in my face, with the wind in my hair, and my arms up in victory!
So now I’m going to listen to my music really loud and dance in front of my mirror until I’m out of breath. But I’ll keep going because I won’t quit.
Over 13 years ago they told me I would die within the year and—look at me now!
Download a FREE copy of the book “Surviving Lung Cancer” now.
In the book you will discover:
Exactly How The Author Has Survived Lung Cancer For Over 22 Years And Counting Conventional & Non-conventional Medicine Secrets How To Make The Right Decisions For Your Health The Secrets To Minimizing Stress Secret Foods & Drinks For Lung Cancer Survivors Secret Mind Hacks For Healing Your Lung Cancer What To Do After Finishing Conventional Treatments
Beating Crazy Odds – A Powerful Cancer Survival Guide is written by a lung cancer survivor who beat a 1.2% survival rate and teaches other cancer patients how he did it!
The book arms patients with vital tools, essential knowledge and powerful mind-body-spirit exercises that complement conventional treatments to help win the fight against cancer, while at the same time developing the skills needed to prevent a re-occurrence.
Endorsed by a Senior Physician at Dana-Farber Cancer Institute and Professor of Medicine at Harvard Medical School, author Lloyd augments what the doctors tell you with critical information they don’t tell you.
It’s a MUST READ for anyone fighting cancer.
The body reacts to our state of mind. By taking a proactive approach, patients learn how to minimize stress, dispel fear and stay positive in the face of adversity in order to help the body heal. Patients also learn how to create their own breathing and visualization techniques to help dissipate tumors by directing the mind, body and spirit to clean and clear specific areas where a tumor exists.
Written by a lung cancer survivor who understands what it takes to beat the odds, this book offers unparalleled hope and direction for anyone facing this illness. It is filled with specific exercises and techniques to promote healing and reverse side effects by taking a proactive approach in helping to restore your mind, body and spirit to an optimum state of health. Endorsed by a Lung Cancer Specialist and Associate Professor at Harvard Medical School, this book combines what the doctors tell you with critical information they don’t tell you.
I am very lucky to have survived such a severe case of lung cancer but it was not by accident. Without a clear path to follow, I had to search through a great deal of material and pull from a variety of sources to assimilate knowledge and develop the skills that I needed to survive.
As I overcame the illness and returned to the cancer center for checkups, I would speak to other patients and family members, explaining what I did, in addition to the chemotherapy and radiation. I cannot begin to express the look in their eyes as they hung on every word. They were starving for direction and extremely grateful to receive advice from a survivor.
It was through these experiences that I realized what I had to offer, not only in the way of hope, but with specific techniques and exercises to help others heal. So I decided to write my first book on the subject, How to Survive Lung Cancer – A Practical 12-Step Plan, published in 2007. Since that time, I have been asked by a number of patients and professionals to expand the book in order to benefit not just lung cancer patients but all cancer patients.
Throughout this period, I also coached individuals and family members with various types of cancer who contacted me for additional help. I co-authored papers with doctors at the University of Virginia and have been asked to speak on several occasions, leading to extended Q&A sessions. The feedback I received helped me to write this new book and teach all cancer patients more clearly how to beat the odds and live a much healthier life, filled with love and joy.
Swarner, as a teenager, needed it in large doses. Nothing is more devastating than finding out, at 13, you’ve got Stage 4 Hodgkin’s Lymphoma and have three months to live.
The journey to self-worth starts with embracing who you are, appreciating your strengths, and believing in your potential. Embrace the struggle, because tough times never last – tough people do! Your journey may be challenging, but remember, it’s shaping you into a stronger version of yourself.
Your purpose may be intertwined with your struggles, as your unique experiences can shine a light for others walking a similar path. LIVESTRONG Films: Sean Swarner. Embrace the opportunity to inspire and uplift others with your resilience by pushing forward. Your journey may inspire others to find strength in their own struggles.
Life is a journey filled with twists and turns, but knowing what you want from it can make all the difference. Take a moment to reflect on your dreams, passions, and goals. When you have a clear vision of what truly fulfills you, you can pave your path to happiness and success. Remember, it’s never too late to chase your dreams and create the life you desire.
Let’s all take a step closer to our aspirations today! Having faced and conquered enormous challenges (Everest with one lung for example).
I know that a positive mindset is the key to overcoming obstacles
and achieving your dreams.
Don’t miss out on transforming your own life! Let’s ignite the power of positivity and achieve the impossible. Your mindset is your ticket to success! Ready to dive deeper? Visit my website for more resources, insights, and join a community of like-minded warriors striving for greatness!
Profound perspective on the power of choosing our outlook on life. Don’t miss out on this eye-opening insight that will change the way you see challenges! Embrace the setbacks and pain.
Learn from them and watch yourself grow stronger than ever before! Stop chasing external approval for happiness! Real joy comes from within, not from the number of likes or nods of approval you get. Own your worth, validate yourself, and watch how true happiness follows.
It was unreal, but the journey was only halfway done! Imagine standing on top of the world, surrounded by a sea of stars at eye level and a breathtaking sunrise. The climb was grueling, but the view from Everest’s summit was beyond words. Reaching the top was just the beginning. Life’s peaks may seem like the ultimate triumph, but often there’s always another mountain to climb. Embracing the challenge, finding strength in adversity, and pushing limits – that’s the essence of life’s climb. Checkout this clip of the man with the stash and myself covering the incredible journey of my summit. We discuss the highs, lows, and the realization that our greatest summits are often disguised as mere milestones.
Before you can light up the world, you must first ignite the fire within. Being whole is the key to achieving the extraordinary. I never imagined I’d conquer what no one in history has done before – summiting the highest peak on every continent, conquering the North & South Poles, and competing in the Hawaii Ironman World Championship. Especially with one lung. This journey taught me that true greatness starts from within. By nurturing your own well-being, you unlock the power to uplift others in ways you never thought possible. Remember, you are the architect of your own success. Prioritize self-care, self-love, and self-discovery. Embrace your strengths, conquer your fears, and watch as the world opens up to endless possibilities.
Your mindset is a FORCE that can shape the course of your life. Dare to break free from limitations, conquer challenges, and unleash your TRUE potential! Embrace the journey of doing the impossible! Let’s push ourselves to become better each day, to do better than yesterday.
Let’s inspire each other to reach new heights and conquer our own ‘impossible’. Remember, every small step forward is progress! Imagine this: You find a letter from your future self. What would it say? Maybe words of encouragement to keep pushing through the tough times, a reminder of how far you’ve come, or a nudge to never give up on your dreams? Let’s all take a moment to reflect on what our future self would want us to know today. Embrace the challenges, enjoy the journey, and keep moving forward with unwavering determination. I’m thrilled to share this sneak peek into my journey and the powerful message that drives me each & every day. From conquering Everest to defeating cancer twice, I’ve learned that anything is possible when we refuse to give up.
Join me as I inspire and motivate audiences around the world to embrace their resilience and reach for their highest potential. Interested in having me speak at your next event? Jump on over to my website & chat with my team!!
Check out my Emmy nominated film “True North” on Amazon! This project was such a powerful & beautiful experience. I can’t wait for you to see it! My hope is that it inspires you to defy the odds, conquer your fears, and push beyond your limits! This film is a testament to the indomitable spirit that resides in every heart, urging us to reach new heights. Your path to greatness begins with the belief that you are capable of achieving the extraordinary. Tag someone who needs a boost of inspiration today and let’s spread the message that greatness knows no boundaries!
Embrace the extraordinary! Why settle for average when you were born to stand out? Don’t blend in with the crowd – dare to be different, dare to be remarkable!
Let’s break free from the ordinary and strive for greatness together!
Success is not always about the new and flashy things. It’s about finding fulfillment in what you do.
Embrace your uniqueness because being different is your superpower!
Health psychologist Kelly McGonigal is here to talk about stress. In particular, she’s here to make the case that stress might not, in fact, be the enemy we tend to think it is. To do this, she asks those assembled in the conference hall in Edinburgh to indicate how much stress they’ve felt in the past year. Surprise surprise, the majority of the audience confesses they have suffered a good deal. Poor stressed lambs at TEDGlobal!
But now, a confession. “My fear is that something I’ve been teaching for the past ten years has been doing more harm than good,” says McGonigal. “Basically, I’ve turned stress into the enemy. But I’ve changed my mind about stress, and today I want to change yours.”
She cites the 2012 study that made her rethink her whole approach, “Does the perception that stress affects health matter?” by scientists from the University of Wisconsin-Madison. It turns out that thinking that stress is bad for you is … really bad for you. Incredibly, she says, over the eight years of the survey, 182,000 people died prematurely from the belief that stress was bad for them. She extrapolates for us: If that estimate is correct, then believing this is so would have been the 15th largest cause of death in the United States.
.
“You can see why this study freaked me out,” she adds wryly.
McGonigal cites another 2012 paper, “Improving Acute Stress Responses: The Power of Reappraisal,” published by scientists at Harvard’s department of psychology, and asks what might happen if we change the way we think about stress. “What if we thought about it as helpful?” she asks. Turns out, treating common stress responses as a positive might even be literally good for the heart. Why not recast the stress response as your body responding usefully to a challenge?
McGonigal also wants to talk about oxytocin, the much-hyped (and maligned) neuro-hormone that she describes as finetuning the brain’s social instincts. Amidst all the hype about the “cuddle hormone” and the much-ridiculed notion that we should snort it to become happier people, one fact we lose track of, she says, is that oxytocin is actually a stress hormone.
“The harmful effects of stress on health are not inevitable,” McGonigal says. “How you think and how you act can transform your experience of stress. When you choose to view your stress response as helpful, you create the biology of courage. And when you choose to connect with others under stress, you can create resilience.”
So while she obviously wouldn’t ask for more stressful experiences in her own life, she does have a new appreciation of the condition. “When you choose to view stress in this way, you’re not just getting better at stress, you’re actually making a pretty profound statement,” she concludes. “You can trust yourself to handle life’s challenges. And you’re remembering you don’t have to face them alone.”
We’re often taught that stress is harmful and best avoided, but The Upside of Stress aims to prove otherwise. Kelly McGonigal argues that stress isn’t the enemy it’s typically made out to be—rather, it’s an ally we should embrace. By changing your mindset on stress, McGonigal claims you can transform it into a resource that leads to enhanced health, greater success, and a more meaningful life.
You’re going to want to read this.
New research finds that when people are subjected to poor grammar, it actually causes them stress — and even initiates a “fight or flight” response.
Heart rate variability — or HRV, which measures the time in between beats — was used as the primary metric to determine how linguistic liabilities impact a person’s physical being.
When relaxed, HRV is commonly less regimented — and it only becomes regular during times of stress, researchers noted.
The more grammatical errors a person heard coincided with the strict regularity of their heartbeat, an indication of stress.
Hearing or reading those cringeworthy errors triggers two (not to or too) pieces of the ANS that are known as the sympathetic and parasympathetic nervous systems.
“Simply put, the sympathetic nervous system activates the ‘fight or flight’ response during a threat or perceived danger, while the parasympathetic nervous system controls the ‘rest and digest’ or ‘feed and breed’ functions of the body,” principal study investigator Dagmar Divjak said.
“Our findings show that [the ANS], too, responds to cognitive demands, and this suggests that cognitive effort reverberates through the physiological system in more ways than previously thought.”
Just over a decade ago, researchers at the University of Illinois commonly connected grammar sticklers to having a form of OCD called Grammatical Pedantry Syndrome. The brain activity of the verbal buffs showed similarities to obsessive-compulsive behavior.
“The results of this study bring into focus a new dimension of the intricate relationship between physiology and cognition,” Divjak said. “The relation between language cognition and the autonomic nervous system has so far received less attention.”
Now, the latest report looks to further pursue evidence that words matter — and may actually hurt us.
“This study provides us with a new method for tapping into aspects of cognition that are not directly observable,” the professor added. “This is particularly valuable in work with language users who are unable to verbally express their opinion due to young or old age, or ill health.”
Navigating the delicate balance between acknowledging emotional triggers and encouraging resilience is essential for healthy interpersonal relationships. Let’s explore this further:
Understanding Triggers and Emotional Responses:
Triggers are stimuli that evoke strong emotional reactions, often tied to past trauma or significant experiences.
When someone says, “You’re triggering me,” they express distress caused by a specific action, word, or situation.
Recognizing and respecting these triggers is crucial.
Effective Communication:
When someone expresses being triggered, listen actively and empathetically.
Validate their feelings by saying, “I understand this is difficult for you.”
Encourage coping strategies and resilience: “Let’s discuss ways to manage these feelings.”
Empathy and Boundaries:
Put yourself in their shoes to respond compassionately.
Indeed, not actively listening to others can indeed lead to stress. When we truly listen, we show empathy and understanding, which can strengthen relationships and reduce tension. If you find yourself feeling stressed, consider practicing active listening by giving your full attention to the speaker and validating their feelings. It’s a small but powerful way to promote well-being.
Feeling disconnected from others can indeed lead to stress. When we struggle to connect with people, it affects our mental well-being. Here are some reasons why you might find it difficult to connect and how to address it:
Negative Experiences: Past negative social experiences can make it harder to trust and connect with others. Consider seeking professional help to work through these feelings.
Over Reliance on Social Media: Spending too much time on social media can lead to feelings of isolation. Try to balance online interactions with face-to-face connections.
Remember, connecting with others is crucial for overall well-being. If you’re struggling, consider reaching out to a therapist or counselor for support.
Sabrina coaches business professionals to finally speak English fluently at Calm English. She believes that language is a tool we can use to reach professional goals and see big, adventurous dreams become reality. If you’re ready to be a successful English speaker, speak English fluently, get the jobs and promotions you deserve and see your life improve with English get started with her free mini-guide to speaking English fluently here.
If you feel stress on a daily basis, the 3-3-3 rule for anxiety can make all the difference.
According to Gallup, 57 percent of American and Canadian workers report that they feel stressed daily. The anxiety that these employees feel is tremendously disruptive–interfering with their ability to engage with their jobs and to work effectively. As a result, it’s in every leader’s interest to help their people dial down the stress and anxiety they feel.
Fortunately, there are some very effective tools available to do just that. Many people have found that the 3-3-3 rule for anxiety can bring relief–allowing them to de-stress and find the balance they need to contribute their best efforts, both on and off the job.
The next time you’re feeling overwhelmed by stress and anxiety, give the 3-3-3 rule for anxiety a try–just five minutes can make a world of difference. And then be sure to teach your employees how to do it. Here’s how it works.
1. Find a quiet space.
When you start to feel stress and anxiety take over, find a quiet space where you can remove yourself from the hustle and bustle and comfortably stand or have a seat. The idea is to remove yourself from distractions (and that includes your smartphone and coworkers).
2. Identify three things you can see.
After you get comfortable, take a look around you and identify three nearby things you can see. One thing might be a smear of paint on the wall, the second could be a trail of ants crossing the floor, and the third might be a window shade gently moving in the breeze. Focus on these three things–one at a time–and closely observe their details.
3. Identify three things you can hear.
After you’ve identified and observed three things you can see, do the same for three things you can hear. Listen carefully and see what catches your attention. One thing might be the dull roar of a distant freeway, the second might be a vacuum cleaner in the office next door, and the third could be the opening and closing of a set of elevator doors. Focus your attention on each of these three sounds–one at a time–studying them carefully.
4. Identify three things you can feel.
Next, move your attention from the things you’re seeing and hearing to the entirety of your body. What do you feel? Pick out three things you can feel and focus on them, one at a time. The first might be a headache that you’ve been nursing all morning, the second could be the tiredness you feel because you stayed up too late the night before, and the third might be a persistent itch on your ankle.
5. Repeat steps 2, 3, and 4 twice more.
Take time to repeat the cycle of seeing, hearing, and feeling two more times. With each cycle, you’ll feel your anxiety dissipating.
6. Take some deep breaths.
After you complete the three cycles of seeing, hearing, and feeling, take several deep breaths. Inhale slowly through your nose–feeling the air move into your body–hold the air in your lungs for a moment, then exhale gently as the air moves back out of your body. By now, your anxiety should be a thing of the past.
7. Reflect.
So, how do you feel? Check in with yourself and compare how you feel now with how you felt before you began this exercise. If you’re feeling less anxious (chances are, that’s going to be the case), then enjoy your new state of mind. If you’ve still got more work to do, then give the 3-3-3 rule for anxiety another try.
And remember, this exercise isn’t just for you. You can teach others how to use the 3-3-3 rule for anxiety for their benefit. Just think of the difference you can make in your organization.
It’s been almost 20 years since I met my first disappearing patient — a nurse in her early 40s, let’s call her Kate. Kate was diagnosed with breast cancer. As a nurse, she had seen the results of breast cancer treatments. She was terrified, and determined. She was not heading for surgery, nor chemotherapy, nor radiation.
But Kate worked in a hospital. She worked with the doctors who diagnosed her cancer, and she worked with the surgeon, who wanted to schedule her into surgery “as soon as possible.”
The first thing Kate did was slow down. She did some research. It didn’t take her long to remind herself that in Canada, and in the USA, the treatments for cancer are akin to law. No hospital would dare deviate from the deadly three (cut, poison, burn).
Kate’s cancer was not large.
She had been tested for cancer last year and no cancer was found. She knew it took many years for cancers to develop. At first, she was furious, “If it is here today, it must have been here last year. Why didn’t you find it last year?” It had not metastasized. It was not growing rapidly and was not affecting her health in any way. In theory, she had lots of time. So, she took some time.
But Kate didn’t look for magic cures.
She didn’t search for the latest “cancer medicine.” She wasn’t interested in curing herself. She knew she was a nurse, not a doctor. She searched instead for the “cured” – patients who were diagnosed with cancer, and no longer had cancer. She knew from her work in the hospital, from conversations with patients, and with some staff, that these people existed — but from the perspective of the medical establishment, they seemed to disappear.
It didn’t take her long to find some patients who claimed they were cured. They hadn’t disappeared from life. They were eating, drinking, loving, and living full healthy and prosperous lives. But according to the medical records, they didn’t exist. They were “never cured.”
The medical system treated their cures as “anecdotal.” It ignored them. There was no attempt by any doctors to understand what happened to these cancer patients. They were no longer sick. The medical system looks after sick patients, treats sick patients. These patients were not sick.
Kate looked and listened.
Her interest was not clinical science vs. anecdotal evidence.
Her interest was personal. She talked, listened, and compared stories. From several, she learned about a clinic that did not claim to cure cancer. It did not use medicines to treat cancers.
But patients were cured, somehow. This clinic was not in Canada. It was not in the USA. She would have to go to Mexico to learn more.
There are lots of alternative treatment clinics in Mexico.
Are some of them valid, using important techniques to cure cancers?
Are some of them scams, wanting to take money from desperate clients?
Do some of them have a cure that works sometimes, but might not work for her?
Kate didn’t know. She did more research. She called the clinic.
The staff did not claim to cure cancer.
Claiming to cure cancer is dangerous, even for a clinic outside of North America. They suggested Kate visit the clinic and see what happens there, no charge for a visit, but she would need to pay for her travel to Mexico. Kate had done her research. She had met and talked to patients whose cancers had disappeared.
Kate made her decision.
She was familiar with cancer diagnosis techniques in Canada.
She had undergone a physical examination, a mammogram, that detected a lump in her breast. Then she had a biopsy, where tissue was taken from the lump and was sent to a lab for analysis. The lab technician tested and examined the sample and issued a diagnosis “cancer” or “not cancer.” Once the diagnosis is issued, everybody swings into action.
Kate knew that the mammogram had a high false positive rate and a false negative rate. Many people who are diagnosed with a “possible cancer” by a mammogram do not actually have cancer. She was also aware that cancer biopsies have a false positive rate and a false negative rate, as well. Her work in the hospital, with real patients, had made this very clear.
They didn’t really know for certain if she had cancer.
Her surgeon, on the other hand, was still pressing her to schedule treatment.
Kate knew one thing. She had time. She cashed out some savings and booked a “holiday” in Mexico.
At the clinic, Kate was surprised that there was no “cancer diagnosis.” They did check the presence and size of the lump on her breast. But they didn’t repeat the biopsy. The clinic read her diagnostic reports, but did not investigate them further. There was instead a very thorough analysis completed by a suite of doctors. It took two full days of tests and interviews, if I remember correctly.
Kate was asked about her family’s medical histories.
She gave blood samples. She was questioned extensively about her diet, about what she eats on a regular basis. What foods does she like and eat often? What foods does she not like and never eat? Doctors examined her lungs, her heart, liver, and other bodily organs with various tests. Her immune system was tested. Extensive interviews about her life, her work, her relationships, and more.
At the time I talked to Kate, I didn’t realize that she was not getting a “medical analysis,” she was actually getting a “healthicine analysis.” Her tests and questions fit perfectly to the hierarchy of healthicine: genetics, nutrition, cells, tissues, organs, bodily systems, body, mind, spirit, and community.
Kate’s genetics were analyzed through family history. There may have been further genetic analysis, I don’t remember all of the details. Her nutritional status was analyzed, not just by analyzing what she ate, and what she preferred to eat, but also by studying what she didn’t like to eat, what she deliberately never ate, what foods she believed she was allergic to. Her cells and tissues were analyzed directly, through blood samples and physical examination, and indirectly through medical history and other tests.
Many of her organs were tested for healthiness.
Her bodily systems, immune system, circulatory system, respiratory system, hormonal systems and more were analyzed and assessed. Her physical body was measured, weighed, and examined. Her mental health was assessed, as well as her spiritual healthiness. She was in good spirits, even in light of a potentially life threatening illness. Her community health was analyzed as well. Her family, her relationships with her children, her spouse, her parents, her work community, and more.
After a few days, Kate met with a group of doctors to discuss her health, not her illness, her healthiness. Diagnosing illness is difficult. Analyzing healthiness is more complex. It took several doctors and several hours for Kate to learn and understand what they had learned about her healthinesses and her unhealthinesses.
They then “prescribed” two weeks, if I remember correctly, of healthiness training, tailored to Kate’s specific situation. She spent the next two weeks at the clinic, learning to be healthier, not learning how to be “healthier in principle,” rather – learning what Kate needed to do to make her diet, her body, her mind, her spirits, and even her relationships with her communities healthier. She could not change her work community. But she could change how she reacted to and interacted with it – to improve her own health. After two weeks of learning at the clinic, her breast lump had started to shrink.
Kate went back to Canada, to put her learning into action.
The lump disappeared. Her diagnosis was still there on paper. But her “cancer” had disappeared. She was retested at her hospital and no cancer was found.
Then Kate began to disappear.
When the surgeon asked again, she explained that she was not going to surgery.
The surgeon looked away. He refused to look her in the eye after that.
But Kate didn’t disappear from her family. She went back to her family. She didn’t disappear from her job. She went back to her job. She disappeared from the cancer system. Her cancer disappeared, so, as a cancer patient, she disappeared.
Was she cured? We don’t know.
There is no useful definition of a cancer cure.
No medical or scientific test that can prove a patient has been cured of cancer. Our cancer treatment statistics have no count for people who are cured of cancer. Patients that are cured, whether they are cured with medicines or not, are not counted. No breast cancer patients are officially cured by medicine. If their cancer goes away without treatment, they disappear from statistics. If their cancer is killed by radiation, chemotherapy or surgery, they are not cured, they are a “survivor.” Everyone knows that cancer survivors are always waiting for the cancer to reappear. Their symptoms are in remission, but their cancer is not cured. They are not cured. With no proof of a cure, it might just be hidden.
Kate no longer has cancer.
She paid, from her own pocket, for her trip to a clinic in Mexico. After the trip, her cancer disappeared. She had medical insurance. But her insurance wouldn’t pay for her trip. Insurance pays for treatments, not for cures. It pays for treatments, even if they fail. But it does not pay for success. Success disappears.
There are two ways for a cancer patient to disappear.
You might be cured by health. Or you might be cured by a medicine that is not approved. In both cases, the medical system will ignore the cure, and ignore the patient.
If it is not curable – it is not a disease, it is a handicap, a disability, a deficiency, or simply an attribute of the person. All diseases can be cured by definition. I have since met several cancer patients who have disappeared, and not just cancer patients. Maybe you have too?
I’ve met more by internet, email, etc.
There is no way for me to determine if a disappeared patient actually had cancer, if their treatment cured their cancer, if their body cured their cancer or if they still have cancer. We can only tell if there is another cancer diagnosis. Nothing can be told from the absence of a diagnosis.
There is no way for any doctor to tell either.
There are no tests for a cancer cure. There is no way to recognize, much less document a cancer cure. There are no statistics for cancers cured. Many cured patients don’t disappear quietly. They speak out. They write books and newspaper articles. They blog. But it doesn’t matter. They still don’t count.
Once cured, they disappear.
The medical system does not study their cases, does not study their diagnosis, does not study their cures. For chronic diseases, like cancer, arthritis, diabetes, heart disease, even obesity, and many more, there are no techniques to document “cured patients.” As a result, there are no statistics for “cured patients” of any chronic illness.
Once they are cured, they disappear.
Health doesn’t cure illness, it disappears.
And medicine doesn’t count people who have disappeared.
Herbal remedies, Vitamin B-17, hyperthermia, cannabis, bio-oxidative therapies, frequency machines, and detoxification are just a few non-toxic treatments that are being successfully used by thousands of people across the globe to treat their cancer.
To learn more, please visit The Truth About Cancer and sign up to the cancer treatments online summit, “The Truth About Cancer: A Global Quest”. In this exclusive 9-part docu-series, more than 100 doctors, scientists, researchers, and cancer survivors join together to give you the real information no one is telling you about cancer, including documented evidence from doctors and scientists around the world, plus insights and solutions for cancer you’ve probably never heard before.
My Mom Not So Long Ago!
They ban books on real cures that have existed for eons, our own gov’t suppresses this on both sides. There have been cancer cures here forever, worst of all they are causing it with their legislation they pass when you dig into it. My mom was cured of advanced, stage 4 small cell lung cancer in Germany through alternative medicine.
They ostracized her here in the mainstream medical system when she came back cancer free and the FBI came to my parents’ house investigating a source of natural supplements they had brought in. They gave her 3 months to live and in less than 3 weeks with these treatments, noon-toxic, she was cancer free and cured. The mainstream system turned their nose up and would not even perform any requested diagnostics.
Of course you do not want to keep doing their mainstream CAT Scans as it reactivates cancer cells with all that radiation. When we requested our own type of lab tests for testing that are non-toxic due to researching and speaking to Dr’s that are true Dr’s and were trained in mainstream and went on to train in other alternative modalities they rebutted our family. Our mainstream medical system is a mafia. Quit giving money to the mainstream system which actually kills you. ~ Shakira Morrison
INTRODUCTION Many individuals—especially older adults—panic when they experience episodes of forgetfulness, wondering whether memory lapses such as forgetting names and losing track of house keys are early dementia symptoms. While it is true that the incidence of dementia increases with age, there are many factors that influence memory ability and cognition that have nothing to do with progressive neurodegenerative diseases such as Alzheimer’s disease and other dementias. Learning more about such issues as how memory works, how and why memory performance changes, and how to increase memory power can help you resist memory decline, and recognize symptoms of memory loss that call for medical assessment.
Genetics accounts for about half of our memory ability—some people may be born with the capacity to easily retain what they learn, while others may have to work harder. The other half of memory is shaped by our environment. Factors such as diet, education, and medical care all combine to affect brain function. If you weren’t blessed with a strong memory, there is evidence that you may be able to improve your memory performance through changes in your lifestyle and behavior.
Memory has three distinct phases: encoding, storage, and retrieval.
Information from your sense organs is transmitted via neurons to the regions of your brain that are associated with vision, sound, smell, taste, and touch. The impulses speed from one nerve cell to another across tiny gaps called synapses. Each of the individual cues is combined into a single memory in a region of your brain called the hippocampus. This process is known as encoding. Next comes the storage phase of the process. Your hippocampus sends the memory to the cerebral cortex, a kind of permanent file cabinet.
There are two distinct mechanisms to memory storage: short-term (working) memory and long-term memory.
Short-term memory involves information your mind stores for immediate recall. Your short-term memory can hold small amounts of information for limited amounts of time, such as remembering a telephone number long enough to find a phone and dial the number. Long-term memory involves retaining information for days, months, or years. The brain can store almost limitless amounts of long-term memory, which is why we can learn so many new things and retain what we’ve learned for many years.
Memories can be retrieved either through recall or recognition. Recall involves directly accessing a memory, such as remembering the name of a book you read a week ago. Recognition involves cues that help you retrieve a memory, such as the process used in school multiple-choice tests.
Studying How Normal Memory Works
Many scientists believe that a memory is formed when a brief pattern of electrical impulses moves through a network of neurons, strengthening connections between the affected brain cells. This leaves a “memory trace” in the brain, which is revived when the information is later recalled. The brain has many different areas, each of which specializes in different types of information. Researchers now know that certain attributes of a memory are grouped with other, similar recollections. For example, the smell of popcorn may be grouped together with remembrances of favorite films. When you recall information, your brain cross-references the many different attributes of that memory. Using techniques like functional magnetic resonance imaging (fMRI) scans, researchers have been able to map connectivity between different brain regions and capture brain activity that indicates where certain memories are created and what the likelihood is that someone will be able to recall that information.
How Memories Are Lost Most
Most memory problems are not related to dementia. In the majority of individuals, the problem stems from physical or emotional issues, or from the normal effects of aging. Dehydration, fever, head injury, low thyroid function, liver and kidney problems, high blood pressure, obesity, poor nutrition, low blood sugar, and reactions to medications all are physical factors that can cause temporary memory impairment. Fortunately, these conditions can be treated. Emotional distress also can have a devastating effect on memory. Repeated stress, sleeplessness, depression, and anxiety can interfere with the normal encoding and storage process, and can significantly affect your ability to remember even the simplest things.
Age-Associated Memory Impairment (AAMI)
In addition to the everyday memory loss caused by physical and emotional factors, aging itself can take a toll on memory. This natural process, called age-associated memory impairment (AAMI), may start as early as our late 20s and progress as we get older.
Changes related to AAMI include:
• Loss of brain cells (neurons). This process usually occurs gradually over time. People who remain healthy and are mentally, socially, and physically active are able to generate new cells to replace many of these lost neurons.
• Reduced levels of certain hormones and neurotransmitters that are involved in the transmission of signals among cells in the brain, and to and from the brain and other parts of the body.
• Brain atrophy. The brain loses both volume and weight with age. This shrinkage is the result of the gradual loss of neurons (the brain’s “gray matter”) and damage to the branch-like dendrites and nerve fibers called axons (the brain’s “white matter”) that extend from the neurons and connect them to other cells.
• Shrinkage of brain tissue on the brain’s surface (gyri), and the grooves on the surface of the brain (sulci) widen. • Increased volume of ventricles (the spaces in the brain that contain cerebrospinal fluid).
• Decreased blood flow to the brain.
• Buildup of toxic proteins. Twisted protein filaments, called neurofibrillary tangles, may form inside nerve cells, and clusters of damaged beta-amyloid proteins, called plaques, may build up in the brain’s gray matter.
The effects of age-associated changes become most apparent after age 50, when people may begin to experience an increase in memory lapses, However, declines in cognitive skills such as reasoning, memory, and vocabulary skills may begin as early as age 45. The older people are, the more difficulty they may have with short-term memory and mental organization. AAMI may cause people to misplace things more easily, occasionally forget a name or phone number, have more trouble multitasking, become easily distracted, or be unable to learn things as easily as they once did.
When Memory Impairment Becomes More Serious
Most people who live into their 70s, 80s, and beyond never experience memory problems more severe than normal age-associated memory impairment. But for some, forgetfulness may get progressively worse and begin to interfere with everyday functioning—important indications that there may be cause for concern. A medical assessment may reveal that the problem is related to a treatable condition. Even when no related health conditions are identified, medications can help improve memory in the early stages of impairment, and ease symptoms such as anxiety or restlessness.
I. WHAT IS DEMENTIA?
Dementia comes in two forms: Primary dementias—such as Alzheimer’s disease or Lewy body dementia (dementia with Lewy bodies, or DLB)—involve damage to or wasting away of the brain tissue. Secondary dementias are memory troubles caused by mental or physical disorders, such as depression or thyroid problems. Changes in brain function with dementia can alter virtually everything about you—including your personality and behavior. According to diagnostic criteria, serious memory lapses may indicate dementia if they are accompanied by at least one other symptom of cognitive decline.
Dementia signs may include:
• Asking the same questions over and over
• Losing the ability to accomplish complex tasks, such as cooking a meal
• Becoming lost in once-familiar places • Forgetting names of familiar people
• Having trouble using language, or putting words together
• Failing to remember regular appointments
• Neglecting personal hygiene—such as brushing your teeth or showering
• Showing signs of mental confusion
• Having difficulty recognizing common objects, like a toothbrush or TV set
• Having trouble coordinating movements
• Experiencing mood symptoms such as anxiety, unusual irritability, or depression.
Mild Cognitive Impairment (MCI)
Scientists are working on identifying dementia in its earliest stages so that treatments can be initiated before brain damage has occurred. They are looking beyond the symptoms of age-associated memory impairment to the next stage in memory impairment, which sometimes—but not always—leads to dementia. Called mild cognitive impairment, or MCI, this stage is characterized by memory loss that is worse than that expected for the person’s age group and forgetfulness that may become increasingly noticeable to others. Currently, as many as 10 to 20 percent of Americans aged 65 and older have MCI, up to 15 percent of whom may progress to dementia each year.
People with MCI have more trouble remembering names or words, performing complex tasks, and acquiring and retaining information. People with MCI also perform worse on cognitive tests than is normal for their age group. People with MCI have normal mental function and can still perform their daily activities. They are able to follow written or spoken instructions, and can take care of themselves—that is, get dressed by themselves, prepare their meals without assistance, and go on walks without getting lost. In Alzheimer’s disease and other dementias, these functions gradually disappear.
Managing MCI
Having MCI doesn’t necessarily condemn you to certain cognitive decline. Many people with MCI won’t progress to dementia, and there are ways to slow the progression of memory loss. You may be able to help reduce your risk for further decline and perhaps even improve your cognition by adopting the lifestyle and behavioral changes recommended later in this report (see Chapter VII).
If you believe you or a loved one may have MCI, consult a health care provider who can help determine whether the memory impairment may be associated with physical or mental issues that are reversible, and recommend treatment.
Reversible Dementia
Just as with age-associated memory impairment and some cases of MCI, dementia can be temporarily caused by medical or psychiatric conditions, such as a high fever, vitamin deficiency, head trauma, or depression. Because many causes of these secondary dementias are reversible with treatment, it’s important to see a doctor if you’re experiencing sudden memory-loss symptoms, especially if your health has recently changed. The following are among the more common reversible causes of memory loss:
Excess alcohol consumption
Beer, wine, and liquor contain ethyl alcohol, a central nervous system depressant that impairs thought processes, motor control, and memory, and slows overall brain activity. Heavy drinking (more than two alcoholic drinks per day), even without alcohol dependency, can be harmful, research shows.
Those who use tobacco and alcohol are at a substantially higher risk for dementia.
Smokers face a 45 percent greater risk for dementia than nonsmokers.
Smoking damages the heart and blood vessels, limiting crucial blood flow to the brain and increasing the risk for stroke. It increases levels of homocysteine—a damaging amino acid that contributes to stroke and dementia risk, and injures the lungs, reducing the supply of nourishing oxygen to the brain. Quitting smoking can significantly reduce the risk for problems with learning, memory processing speeds, and working memory.
Inflammation
Infections that cause brain inflammation, particularly meningitis (an infection of the membranes surrounding the brain and spinal cord) and encephalitis (an A infection affecting the brain tissue itself) can contribute to mental decline if they’re not treated quickly and effectively.
Depression
Long-term chronic depression alters levels of key brain chemicals such as serotonin and norepinephrine, slows activity in the parts of the brain associated with executive function and perception, and shrinks the hippocampus (the part of the brain where memory is processed). Untreated depression is associated with a higher risk for dementia. Seek professional advice if you experience symptoms of depression, which include feelings of sadness and hopelessness that last for two weeks or longer, changes in sleep and appetite, restlessness, fatigue, irritability, a loss of interest in activities you once enjoyed, confusion, impaired memory, and trouble focusing.
Drug effects and interactions
Certain classes of prescription and over-the-counter drugs, including antidepressants, sleeping pills, anti-anxiety drugs, anticholinergic drugs, and some antihistamines, are known to affect memory and brain function. Chemotherapy or radiation for cancer may also cause memory loss, confusion, and difficulty concentrating—a short-term phenomenon that has been termed “chemo brain.” Older adults are especially vulnerable to cognitive side effects of drugs because of age-associated changes in the brain that heighten sensitivity to medications, and changes in metabolism and reduced liver and kidney function linked to aging. Check with your doctor if you recently began taking a new medication or switched to a higher dose of an existing medication and are experiencing memory problems. Drug-related memory impairment is usually resolved by switching medications, changing the dose, or stopping the problem drug entirely.
Lung problems
Conditions that impair respiratory function—such as chronic obstructive pulmonary disease, fibrosis, asthma, and even allergies—can reduce the delivery of oxygen to the brain, impairing memory performance. Treatment can help reverse these effects and, in some cases, may also lower long-term risk of more serious memory impairment.
Metabolic disease or abnormalities
Certain metabolic diseases can wreak havoc on your memory, and require assessment and advice from medical professionals.
These include:
Abnormal thyroid function
An underactive (hypothyroidism) or overactive (hyperthyroidism) thyroid gland has been linked with impairments of memory, visuospatial organization, attention, and reaction time. Even subtle variations in thyroid function can cause significant cognitive effects.
Metabolic syndrome
This condition involves a cluster of risk factors that include abdominal obesity, low levels of HDL cholesterol, high triglyceride levels, high blood pressure and insulin resistance. In insulin resistance, the body doesn’t respond appropriately to insulin produced by the pancreas, impairing the ability of glucose to leave the blood and enter the cells as it should. The pancreas produces more insulin to compensate, and this excess insulin can lead to inflammation and damage to the brain.
Diabetes
Diabetes—a disease in which the body cannot use glucose (sugar) properly, resulting in higher-than-normal blood sugar levels—may hasten cognitive decline by contributing to hardening and narrowing of blood vessels (atherosclerosis), which can reduce or block blood flow to brain tissue and deprive brain cells of necessary oxygen and nutrients. Depending on where the blockage in the blood vessel occurs, memory can be affected. Some studies suggest that diabetes may be associated with atrophy in the brain’s frontal lobes (responsible for attention and long-term memory) and temporal lobes (responsible for language skills and memory of verbal and non-verbal information).
Sleep problems
Optimal memory performance requires about seven hours of sleep each night. Research suggests that chronic sleep deprivation is associated with memory loss and may increase the risk of developing dementia by as much as 30 percent. Older adults who wake up frequently during the night are more likely than sound sleepers to have amyloid markers in their spinal fluid and amyloid plaque buildup in their brains—both indicators of Alzheimer’s disease. Be sure to get treatment for reversible conditions that can disrupt sleep and may be linked to memory problems, which include:
• Anxiety and/or depression
• Obstructive sleep apnea (OSA), a condition sometimes associated with obesity in which the muscles in the upper airway that support the soft palate, tongue, and other structures relax and collapse, blocking the air passages and causing temporary cessation of breathing
• Restless legs syndrome (RLS), which interferes with sleep by causing unpleasant sensations in the legs that occur just before falling asleep or during the night.
Stress
Stress increases the brain’s release of the hormone cortisol, which can damage both the hippocampus and neurons, promoting memory problems. The brain effects of excessive levels of cortisol are reversible, but not if the stress continues for months or years. Learning how to manage your stress and anxiety is important for keeping your memory functioning at its peak.
Vitamin deficiency
As you age, your rate of nutrient absorption slows, making it harder for your system to get the essential vitamins it needs. Drinking and smoking exacerbate this problem by leaching nutrients from the body. Vitamin deficiencies that affect brain function include a lack of the B vitamins.
A deficiency of vitamin B12 is associated with pernicious anemia that can damage brain cells and lead to symptoms similar to those of dementia; B6 and folate, which help promote healthy nerves and red blood cells; and vitamin B1 (thiamine), a deficiency of which can, over time, interfere with the ability to create new memories.
People with a B vitamin deficiency often have elevated levels of the amino acid homocysteine, which is damaging to brain cells and blood vessels. The B vitamins are found naturally in animal-sourced foods (meat, fish, poultry, eggs, and dairy products) and in fortified cereals, beans, and dark green vegetables.
Another vitamin deficiency with effects on the memory is lack of vitamin D.
Up to 70 to 80 percent of people older than 75 are thought to be deficient in this vitamin, a hormone produced by the action of ultraviolet light (UVB) on the skin that nurtures the development of the brain and nerve cells and protects them against injury. Low blood levels of vitamin D are associated with worse performance on cognitive tests and higher risk for Alzheimer’s disease. Spending as little as five to 30 minutes getting unprotected sun exposure a couple of days a week can help provide adequate vitamin D. The vitamin can also be consumed in supplement form or in foods such as fish liver oils, fatty fish, fortified dairy products, and cereals.
Irreversible Dementia
Some dementia types are associated with brain damage that is irreversible. These are known as primary dementias, the most common of which is Alzheimer’s disease (AD). Apart from AD (which will be covered at greater length in a separate section), the following are important causes of primary, progressive dementia: Vascular dementia (VaD)
Many conditions that adversely affect the heart can damage the brain and nervous system and increase the risk of memory decline. Cardiovascular and cerebrovascular diseases are the prime actors in VaD, the second most common form of dementia after AD.
Causes of VaD include:
Strokes and transient ischemic attacks
Strokes involve the blockage or rupture of the brain’s blood vessels, which starves brain cells of oxygen and nutrients.
Damage may occur from one large stroke, a milder stroke called a transient ischemic attack (TIAs, or “mini-strokes”) with symptoms that disappear within an hour or so, or over time, as the result of a series of imperceptible tiny mini-strokes that progressively destroy small sections of brain cells. Damage that affects regions of the brain involved in learning and memory can lead to vascular dementia.
Signs of stroke require immediate medical care, and include the following:
• Sudden numbness or weakness of the face, arm, or leg, especially on one side of the body
• Sudden confusion, trouble speaking or understanding
• Sudden trouble with vision in one or both eyes
• Sudden trouble walking, dizziness, loss of balance or coordination
• Sudden severe headache with no known cause.
Although TIAs usually do not cause permanent damage, they require prompt attention to reduce the risk of another, more serious stroke. With multiple tiny mini-strokes, symptoms may appear gradually over time as the damage spreads, and can include memory loss, shuffling movements, inappropriate behavior, and loss of bladder or bowel control.
It’s not possible to reverse the damage caused by a stroke, TIA, or other forms of VaD; however, you may be able to avoid further injury to brain cells by lowering cardiovascular risk factors through simple lifestyle changes. Controlling blood pressure and cholesterol, losing weight, quitting smoking, and managing conditions such as diabetes, abnormal heart rhythm, and coronary artery disease can reduce the risk of vascular events.
Atrial fibrillation (Afib)
One in 20 people over age 65, and one in 10 over 80, has Afib, an abnormal heart rhythm in which chaotic pumping actions cause blood to pool, dramatically increasing the risk for brain-damaging strokes and AD. Treatment for Afib usually includes medication, such as drugs to slow the heart rate and blood thinners to reduce the risk of blood clots; cardioversion, which uses electrical pulses or drugs to restore an erratically beating heart to its normal rhythm; and more rarely, catheter ablation, which burns off heart cells that are producing the abnormal rhythm.
Lewy Body Dementia (or Dementia with Lewy bodies—DLB) DLB is the third most common form of dementia, after AD and vascular dementia, representing between 10 and 25 percent of dementia cases. This condition is characterized by the buildup of abnormal proteins called Lewy bodies inside neurons in areas of the brain responsible for memory, language, and consciousness. These same proteins are found in the brains of people with AD and Parkinson’s disease (PD). People with DLB often develop Parkinson’s-like symptoms—including rigid muscles and a shuffling walk—along with other symptoms, such as confusion, trouble thinking and reasoning, hallucinations, and delusions.
Although no cure exists for DLB, medications can help control Fronto-temporal dementias (FTD) This spectrum of disorders (also known as Pick’s disease) causes atrophy of parts of the frontal and temporal lobes of the brain, which control memory, personality, and language skills. FTD may account for up to 15 percent of all dementias, and up to 50 percent of dementias in people younger than 65. Symptoms of FTD tend to come on slowly, and typically involve inappropriate behavior, difficulty finding the right words, and personality changes. In its late stages, FTD resembles AD, with significant memory impairment. Although no treatment for FTD exists, antidepressants and antipsychotic drugs may help control the behavioral symptoms.
Parkinson’s disease dementia (PDD)
PDD is a dementia type associated specifically with the movement disorder Parkinson’s disease, which is characterized by muscle rigidity in the limbs, tremors and balance difficulties, abnormal deposits of proteins known as Lewy bodies, and the hallmark plaques and tangles of AD. An estimated 50 to 80 percent of people with Parkinson’s will eventually develop PDD. As with other forms of dementia, PDD gets worse over time. It’s important to note that many of the drugs used to treat PD, including anticholinergic drugs and L-dopa, can potentially cause or worsen cognitive, mood, and thought disorders (e.g., hallucinations and delusions). Working closely with a doctor can help people with PD find the drug with the highest benefit in proportion to risk.
When to Seek Help
Everyone has a mental slip from time to time, but negative mental changes that are recent, growing worse, and showing no signs of improvement over the course of weeks or months may be an indication of serious cognitive problems. Individuals who suspect that they may have dementia should seek a thorough assessment from a family doctor or internist, or arrange to see a specialist such as a neurologist, geriatric psychiatrist, geriatric psychologist or geriatrician. Even if an irreversible form of dementia is diagnosed, it is possible to treat the physical and behavioral problems associated with the condition, and to get help coping with it.
II. ALZHEIMER’S DISEASE
Despite years of research, scientists still don’t know exactly what factor or combination of factors sets the Alzheimer’s disease process in motion. Understanding this process could help lead to earlier diagnosis and treatment.
The Search for Causes of Alzheimer’s
Among the theories scientists are working on to explain the Alzheimer’s disease process are the following:
Amyloid Hypothesis
The amyloid hypothesis suggests that toxic beta-amyloid plaques (sticky clusters of the protein that accumulate between nerve cells) somehow initiate the brain cell destruction observed in AD. The brain normally produces and then eliminates amyloid protein fragments, but in AD, the removal process is impaired and the protein accumulates and forms sticky masses, or plaques, which destroy neurons and cause the gradual loss of brain tissue.
Twisted fibers of abnormal tau protein called neurofibrillary tangles that accumulate within neurons form the basis of the tau hypothesis, another important theory of AD causation. Normally, tau protein builds part of a cellular structure called a microtubule, which helps transport nutrients and other substances from one part of the nerve cell to another. When tangles form, the microtubules break down, leading to deterioration in this transport system and, eventually, to cell death.
Oligomers
Because treatments aimed at reducing the accumulation of plaque in the brain have not improved symptoms of dementia thus far, some scientists are focusing on clumps of beta-amyloid and tau in the brain called oligomers. Beta-amyloid oligomers are thought to disrupt neuronal communication by changing the structure of communication points between brain cells known as synapses, and by promoting the development of neurofibrillary tangles.
A research study using immunotherapy to target tau oligomers in an animal model of AD both reduced levels of tau oligomers and reversed memory declines. Surprisingly, the treatment also reduced levels of beta-amyloid oligomers, suggesting the two types of oligomers may work in concert to damage the brain.
Cholinergic Hypothesis
The cholinergic hypothesis, the foundation for one of the main Alzheimer’s drug treatments, suggests that AD symptoms result from a decrease in production of the neurotransmitter acetylcholine, which is essential for learning and memory formation. Acetylcholine production is known to decline with age, but AD is associated with a much more significant decline in acetylcholine levels.
Excitotoxicity
The excitotoxicity holds that an over-activation of receptors for the neurotransmitter glutamate causes AD nerve damage. Glutamate is normally responsible for making neurons “fire” as they relay messages through neuronal networks, and is involved in establishing long-term memories. When normal glutamate processes are disturbed, excessive amounts of this chemical messenger build up in the space between brain cells, attaching to the cells, overstimulating them, and eventually killing them.
Oxidative Stress
Oxidative stress occurs when unstable molecules called free radicals, generated by factors such as environmental toxins, stress, and aging, overwhelm the body’s natural antioxidant defense system. As a result, the body falls behind in its repair of cellular damage. Research suggests high levels of free radicals and oxidative stress are among the earliest changes that occur in AD, however oxidative stress may be a marker of AD rather than a cause.
Inflammation
Inflammation has also been proposed as a root cause of AD. The immune system relies on inflammation to combat viruses, cancers, and other dangerous invaders. But when inflammation persists, it can damage neurons and may trigger excessive production and accumulation of beta-amyloid in the brain. AD has been linked to strokes, head injury, and surgery, which can cause inflammation in the brain, as well as to infections that lead to body-wide inflammation. However, treating people with anti-inflammatory medications in the early stages of AD has thus far not been effective at slowing or preventing the disease.
Insulin Abnormalities
The hormone insulin ferries sugar from the bloodstream into the cells to be used as energy or stored for future needs. In people with diabetes, the body either doesn’t produce insulin, or can’t use it effectively, leading to a buildup of sugar in the bloodstream and resulting damage to organs such as the kidneys and eyes. Researchers have discovered that insulin levels drop significantly in the early stages of AD, and progressively decline as the disease advances. Cell death and neurofibrillary tangles appear to be linked to abnormalities in insulin signaling. The theory has led to suggestions that AD may be a type of diabetes. Recent investigations into whether giving insulin to people with early cognitive impairment might slow this decline have been promising.
Alzheimer’s Stages
People who have Alzheimer’s typically go through a series of stages characterized by gradually worsening symptoms, although not everyone will go through all of the stages nor progress through them at the same rate.
Early-Stage (mild) Alzheimer’s
As AD progresses, the individual may remain independent, but encounters greater difficulty handling multi-step tasks, such as following a complicated meal plan, and may need help paying household bills. Family and friends might notice signs like forgetting familiar words or trouble recalling current events. The person may become increasingly withdrawn in social situations, and exhibit personality changes, irritability, anxiety, or depression, putting a strain on relationships with others.
Mid-Stage (moderate) Alzheimer’s
This is the longest stage of AD, and it is the time when assisted care usually becomes necessary. The person will be unable to remember important information, such as his or her address or phone number. He or she will need help picking out clothes and remembering the date and time. The person may become confused or delusional at times and express irrational fears—for example, that someone is stealing from him or her.
Severe (late-stage) Alzheimer’s
Cognitive ability becomes seriously compromised at this stage, as the person becomes unable to communicate or interact with his or her environment. He or she will need help performing even the simplest tasks, such as using the bathroom or eating, and often loses the ability to recognize loved ones. Although medications may help slow the progress of AD, the disease is still incurable—and irreversible. However, treatments and support systems can significantly improve quality of life for people with the disease.
Risk Factors for Alzheimer’s
The overall risk for developing Alzheimer’s is 10 to 15 percent. Older age is a major factor in the disease, with risk doubling about every five years after the age of 65. By age 85, nearly half of all older adults have AD. There’s little you can do to hold back time, but you can reduce your AD risk by addressing a number of other factors that increase your odds of developing the disease (see chapter 7 of this report). These include:
High Blood Pressure
Uncontrolled high blood pressure (hypertension) increases risk for stroke—a blockage in the brain’s blood supply that can lead to disability, problems with thinking and memory, and dementia. Even smaller strokes (mini-strokes or “silent” strokes) that don’t cause symptoms can lead to memory deficits by creating small areas of dead brain cells that can have a significant and lasting impact on memory. By some estimates, one-quarter of people over age 70 have had a silent stroke. Managing stroke risk factors can help preserve brain function.
Cardiovascular Disease
People with cardiovascular disease and heart conditions such as atrial fibrillation and chronic heart failure may be at significantly higher risk for cognitive impairment. The brain relies on a steady stream of oxygen and nutrient-rich blood from the heart to keep it functioning optimally, and the greater the disruption in blood flow, the greater the decline in cognitive function. Preventing and treating cardiovascular disease and its risk factors can combat mental decline.
Insulin Resistance and Diabetes
Insulin resistance, in which the body’s cells become less sensitive to the effects of insulin and have trouble using sugar for energy, is associated with high insulin levels that are thought to be a major factor in the development of Alzheimer’s disease. About 40 percent of older Americans have insulin resistance. The same enzyme that breaks down insulin also breaks down the beta-amyloid protein. When insulin levels are high, the enzyme is occupied with breaking down insulin and can’t efficiently clear out beta-amyloid proteins, leading to the brain deposits that are a hallmark of Alzheimer’s disease.
High blood sugar from insulin resistance is a risk factor for metabolic syndrome—a cluster of conditions that includes an enlarged waistline, high triglyceride levels, low HDL (“good”) cholesterol levels, and high blood pressure—and a characteristic of diabetes, both of which can increase risk for memory loss in older people. It is important for people with diabetes to manage the disorder with diet and medications, and to have their cognitive abilities monitored for signs of decline.
Head Injury
A blow or jolt to the head can cause the brain to shift and bend inside the skull, injuring nerve cells. These traumatic brain injuries (TBIs), which include concussions, not only lead to impairment in the area where damage occurs, but might also lead to the formation of beta-amyloid deposits in the brain.
Head injury can increase risk for Alzheimer’s disease—particularly in older people.
Depression
Individuals with depression, which affects an estimated 6.5 million seniors in the U.S., are vulnerable to all types of mental decline, including vascular dementia and Alzheimer’s disease.
Symptoms of depression include feelings of hopelessness and helplessness, loss of appetite, lack of interest in activities once enjoyed, confusion, social withdrawal, sleep problems, and delusion. In older adults, these symptoms can mimic those of dementia. Depression at any age can be addressed with treatments such as antidepressant medicines and talk therapy.
Poor Diet
An unhealthy diet that is high in fat and low in important nutrients can lead to chemical changes in the brain, accumulation of excess abdominal fat, high blood pressure, and high insulin levels, among other effects. These risk factors may, in turn, contribute to health conditions such as diabetes and stroke, which have been directly associated with increased Alzheimer’s risk. Eating a diet that promotes both heart and brain health may have a protective effect, shielding against the cumulative damage that leads to dementia.
Smoking
Research suggests that current smoking impairs memory function and increases the risk for dementia by 50 percent. Nonsmokers who are exposed to secondhand smoke face a 44 percent increased risk of dementia. Smoking is thought to affect memory by contributing to cardiovascular disease, a known risk factor for dementia. The tobacco habit also can damage brain cells and stop new cells from forming. Smokers who quit lower their risk for these conditions significantly.
Mental Inactivity
A lack of mental stimulation can be detrimental to cognitive functioning, and may increase risk for dementia. Studies suggest that older adults who often engage in mentally stimulating activities, such as games, puzzles, classes, hobbies, social interactions, and language training, are more likely to stay sharp than those who are mentally inactive.
Stress
Excessive or chronic stress can heighten risk for memory problems, research suggests, most likely because of an association between increases in the hormone cortisol during stressful experiences and damage to synapses in the brain that relay messages among brain cells.
Genetics
Your genetic background plays a role in your AD risk profile. The more family members you have who are affected by Alzheimer’s, the more likely you are to develop the disease.
Researchers have linked a number of single-gene mutations with the early-onset (before age 60) form of Alzheimer’s, which affects fewer than 5 percent of people with the disease. But finding the genetic factors related to late-onset Alzheimer’s has been more challenging.
Researchers have identified one gene variant—apolipoprotein E4 (ApoE4)—that appears to increase a person’s risk for developing the disease. Although ApoE4 does not cause Alzheimer’s, it impairs the ability to degrade toxic beta-amyloid, and may lead to more rapid loss of nerve cell functioning in the frontal lobe of the brain, a region involved in higher mental functioning.
People who inherit two copies of ApoE4 have a greater risk of developing Alzheimer’s than those who have just one copy. However, because not all people with Alzheimer’s have this ApoE4 genetic variation, and not all people who have the variation will develop the disease, testing for it is not currently considered a useful predictive tool
III. DETECTING ALZHEIMER’S
Although no definitive test for Alzheimer’s yet exists, researchers have learned much more about how the disease begins and progresses. In recent years, scientists have found new ways to diagnose Alzheimer’s disease while it’s still in its early stages.
Diagnosing Alzheimer’s
Individuals who have developed signs of dementia usually begin by seeing a general practitioner for assessment. The physician may make a diagnosis, or refer the person to a neurologist, psychiatrist, psychologist, or other specialist.
An Alzheimer’s diagnosis is usually arrived at by eliminating other possible causes of dementia. Assessment typically involves a physical exam, along with a review of the patient’s symptoms, medical history, and current medications. Even if another cause for the dementia is not found, diagnosing and managing conditions such as infection, high blood pressure, cardiovascular disease, depression, and other problems that can compromise brain function are an important aspect of dementia treatment.
Usually, blood and urine tests are ordered to rule out medical conditions that cause memory loss, such as thyroid problems, kidney or liver dysfunction, or Your doctor may give you simple memory tests, such as the Memory Capacity Test or the Face Name Associative Memory Exam (FNAME).
One or more diagnostic and cognitive function tests may also be recommended, including such instruments as the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment test (MoCA), and the Mini-Cog. Neurological tests (which include assessing balance, coordination, eye movement and reflexes) may be used to look for possible brain disorders, such as stroke or Parkinson’s disease.
Brain scans using high-tech imaging with computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), and functional MRI (FMRI) are often ordered to help identify strokes, bleeding, or deposits of toxic proteins in the brain, abnormalities in brain structure, or abnormal brain activity.
Alzheimer’s Test Options
A clinical diagnosis can pinpoint Alzheimer’s with more than 90 percent accuracy. But researchers are working to identify new ways of detecting this disease in its very initial stages and distinguishing it from other forms of dementia. Earlier diagnosis will help ensure that as new and better treatments become available, patients can benefit from them before their brain has been irreparably damaged.
Brain imaging is an increasingly important way to look for signs of AD in the living brain, and new neuroimaging techniques are under development that are steadily improving these processes. In addition to brain scanning, other new tests that show promise for detecting very early indications of AD include: Biomarkers in cerebrospinal fluid
Proteins released into the cerebrospinal fluid (CSF, the fluid that surrounds and protects the brain and spinal cord) can help doctors identify indicators of damage. For example, researchers have discovered that people with early-stage have increased levels of tau and beta-amyloid proteins in their CSF. Examination of the CFS is an invasive test, which is performed using lumbar puncture or spinal tap to obtain spinal fluid.
Biomarkers in blood or saliva
Certain proteins—including tau and beta-amyloid—may be present at higher levels in the blood and saliva of people with Alzheimer’s. A simple blood test can reveal these biomarkers in the bloodstream. In a recent study, researchers used a technology called liquid chromatography-mass spectrometry to identify unique substances present in the saliva of people with AD, but not in healthy adults.
Sensory changes
Abnormalities affecting sensory organs are often early signs of AD, and might be useful in making a diagnosis, but they must be clearly distinguished from other medical problems that can cause similar sensory changes before they can be fully relied upon as a diagnostic technique. For example, researchers have discovered that impaired smell is linked to elevated beta-amyloid levels, as well as to greater brain cell death. Other studies have found that, compared to healthy individuals, people with AD show signs of eye changes, such as reduced blood flow and cell loss in the retinas of the eyes, and alterations in the retinal nerve fiber. Problems with contrast sensitivity, visual field, depth, motion, and color perception can also indicate Alzheimer’s.
Alzheimer’s prediction methods
Researchers have developed an Alzheimer’s prediction method that involves assigning a score to each of the following risk factors: age, education, gender, systolic blood pressure, body mass index, blood cholesterol, and physical activity. Results suggest that people at high risk for developing dementia within the following 20 years can be identified by combining the scores, and can then implement lifestyle changes that will lower their risk.
IV. TREATING ALZHEIMER’S
To date, no treatment has been found that can halt the progress of Alzheimer’s disease or prevent its destructive effects. Yet treatments are available to relieve some of the most troubling symptoms of Alzheimer’s, and make life easier for both those with the condition and their caregivers.
Alzheimer’s Medications
Drugs used to treat Alzheimer’s can be divided into two categories. One category treats memory, language skills, and other cognitive symptoms of the disease, while the other addresses agitation and other behavioral issues.
Treating cognitive symptoms
Cholinesterase inhibitors and memantine (Namenda) both treat cognitive symptoms of Alzheimer’s.
Cholinesterase inhibitors
These drugs boost levels of a brain chemical called acetylcholine, a neurotransmitter essential for proper memory function that is reduced in people with Alzheimer’s disease. The drugs in this class appear to be about equally effective at improving cognition and ability to function and may also slow the progression of mild-to-moderate Alzheimer’s in about half the people who take them.
The most widely used cholinesterase inhibitors include Donepezil (Aricept), Rivastigmine (Exelon), and Galantamine (Razadyne). NMDA (N-methyl-D-aspartate) receptor antagonist Another drug, memantine (Namenda), is approved to help with memory, attention, reason, language, and other impairments related to Alzheimer’s. The drug regulates the action of a chemical messenger in the brain called glutamate, which in excess can damage nerve cells.
When used alone or with a cholinesterase inhibitor, memantine can delay Alzheimer’s progression and improve cognitive function in some patients. Treating behavioral symptoms Behavioral and psychiatric symptoms such as anxiety, agitation, hallucinations, delusions, aggression, hostility, and uncooperativeness are among the biggest reasons why people with Alzheimer’s are institutionalized.
No drug is FDA-approved for treating behavioral symptoms in people with AD, however, several are used off-label, including: Antidepressants and anxiolytics Antidepressants known as selective serotonin reuptake inhibitors (SSRIs) are the class of drug used to manage symptoms of depression, and they can also ease irritability and depression in people with Alzheimer’s.
These types of antidepressants include citalopram (Celexa), fluoxetine (Prozac), paroxetine (Paxil), sertraline (Zoloft), and trazodone (Desyrel). Although these medicines can sometimes contribute to memory loss, older adults with AD and symptoms of depression who are continuously treated with antidepressants may have less cognitive decline than those whose depression is not treated or is treated only intermittently.
Doctors also use a class of medicines called anxiolytics to address symptoms like anxiety, restlessness, and disruptive behavior.
These drugs include lorazepam (Ativan) and oxazepam (Serax). Some research associates higher mortality with the use of these drugs in dementia patients. Antipsychotic medications Among the most disturbing features of dementia are severe emotional symptoms, such as aggression, hostility, anger, hallucinations, and delusions. These symptoms are so distressing that many doctors prescribe antipsychotic medications—such as aripiprazole (Abilify), clozapine (Clozaril), haloperidol (Haldol), olanzapine (Zyprexa), quetiapine (Seroquel), risperidone (Risperdal), and ziprasidone (Geodon)—in an effort to alleviate them.
Yet recent research has called into question the value, and safety, of antipsychotic use in people with dementia. Studies have found that those taking antipsychotic drugs are significantly more likely to die than those not taking the drug and that the risk of death goes up as the drug dose increases. The FDA has issued a “black box” warning, advising of the increased mortality risk among dementia patients who use these medications. Other drugs have been used as alternatives to antipsychotics, and have been shown to help soothe some agitated individuals.
These might include cholinesterase inhibitors, antidepressants, anti-epileptic medications such as divalproex (Depakote), and lithium. If severe behavioral problems, such as hallucinations, delusions or aggression, don’t respond to other therapies, it may be necessary to prescribe antipsychotic drugs in the short term until other, less risky strategies can be found.
Non-Drug approaches In many cases, non-drug approaches to behavioral and psychiatric symptoms can be just as effective as drugs. These approaches involve calming the agitated person by such strategies as: avoiding potentially upsetting situations; allowing for some agitation, provided it does not pose a risk; or responding flexibly through changes in routine and environment.
Alternative Treatments Researchers have studied a number of possible therapies besides prescription medications for relieving AD symptoms, and have found indications that some may help people with AD. However, more research is needed to clearly establish the benefit of some of these treatments.
Cognitive stimulation therapy
Cognitive stimulation therapy (CST) involves a series of sessions in which the person participates in a variety of mentally stimulating activities designed to preserve cognitive function. Research finds that CST significantly improves cognitive functioning and quality of life among people with dementia, and it may work as effectively as medication.
Nutritional supplements
It’s important to be cautious and consult your doctor before using any type of supplement, since their benefits have not been clearly established. Supplements are not regulated by the FDA and can sometimes cause side effects. Moreover, the potency and purity of supplements are not guaranteed. Alternative therapies that have been looked at—but not definitively proven to be of benefit for treatment of AD—include:
Coenzyme Q10 (CoQ10)
Coenzyme Q10 (CoQ10) is an antioxidant made naturally by the body, that is essential for cellular energy production and for controlling cell-damaging free radicals created as a byproduct of that energy production;
Ginkgo biloba
Ginkgo biloba is an herbal supplement with antioxidant and anti-inflammatory properties commonly used in Europe to treat Alzheimer’s.
Huperzine A
Huperzine A is a natural cholinesterase inhibitor derived from moss that has been used for centuries in Chinese traditional medicine to treat memory problems. Omega-3 fatty acids Omega-3 fatty acids are found in food sources such as fatty fish, walnuts, and flaxseed—help modulate the structure of nerve cell membranes and are important to gene expression in the central nervous system.
Alzheimer’s disease is strongly correlated with a decrease in omega-3 levels in the brain and peripheral tissues. Although there are many reasons to include omega-3-rich foods in the diet, recent research suggests that supplements have no significant effect on cognitive function.
V. ON THE HORIZON: AN ALZHEIMER’S CURE?
In February 2015, the National Institutes of Health acknowledged the importance of finding new treatments for AD by releasing a landmark plan to transform the face of Alzheimer’s disease research. The plan is intended to provide increased support for efforts to learn more about the underlying causes of the disease, and explore ways to treat, prevent, and perhaps even reverse Alzheimer’s disease.
Drugs in the Pipeline
Scientists are incorporating recent advances in molecular biology, bioengineering, genetics, and other fields into research aimed at modifying the outcome of Alzheimer’s disease and finding new possibilities for the treatment of memory disorders and dementia.
Some intriguing examples: Immunotherapy—Alzheimer’s vaccines One of the most exciting, and best-studied new therapies for Alzheimer’s harnesses the body’s own immune system, using vaccines or antibodies to find and destroy beta-amyloid and clear out plaques in the brain, or eliminate the clumps of tau protein (neurofibrillary tangles) that kill neurons responsible for memory loss.
Two types of immunotherapy are under investigation:
• Active immunotherapies, which induce a response from the patient’s own immune system;
• Passive immunotherapies, which involve the administration of antibodies to create an immune response.
Scientists are targeting the accumulation of beta-amyloid proteins using both active and passive immunotherapies.
A few active therapies have produced antibody responses to beta-amyloid, including vaccines known as CAD106, ACC001, and AFFITOPE, all of which are in ongoing trials.
Passive immunotherapy research focuses on drugs called monoclonal antibodies to target beta-amyloid proteins.
These drugs, which are already used to treat cancer, are engineered in the laboratory to mimic the antibodies the immune system naturally produces when confronted by bacteria, viruses, and other foreign invaders.
Genes code for the production of proteins throughout the body. When genes work the way they should, the body functions optimally. But abnormal changes in genes can set in motion a cascade of cellular processes that leads to diseases like AD. Researchers are looking for ways to target these processes using gene therapy.
For example, in a recent study in mice, researchers injected a gene into a key memory region of the brain called the hippocampus.
The gene, which produces a protein involved in long-term memory, reversed memory loss in the animals.
In another study, gene therapy was used to increase nerve growth factor (NGF) production in the brain, which improves neuron survival.
Researchers are hopeful gene therapy will eventually lead to new therapeutic approaches to AD. Histone Deacetylase (HDAC) inhibitors Drugs called histone deacetylase (HDAC) inhibitors target a group of 11 HDAC enzyme expressions of key proteins in the brain. One enzyme in particular, HDAC2–which silences genes that are needed to form new memories–is overproduced in the brains of people with Alzheimer’s. When an inhibitor is used to shut off the gene in the hippocampi of mice genetically engineered to develop Alzheimer’s, it restores normal cognitive function.
Another HDAC inhibitor, used to target HDAC6, reduced brain tau levels and restored memory in mice with Alzheimer’s. Insulin Insulin, the hormone that helps the body convert dietary sugar to energy, is thought to have strong links to Alzheimer’s disease. Because the same enzyme breaks down both insulin and beta-amyloid, a disruption in insulin signaling in the brain can affect amyloid removal, cell survival, inflammation control, blood vessel function, and other factors involved in the development of AD. Researchers are testing an insulin nasal spray they hope might help with Alzheimer’s and other forms of dementia.
VI. HELPING YOURSELF: HOW TO INCREASE MEMORY POWER
Even for individuals who are showing signs of memory difficulties, dementia is not a foregone conclusion. There is good evidence that by being proactive, you lower your risk for dementia or slow the progress of mental decline.
Ways to Lower Your Dementia Risk
Both those risk for Alzheimer’s and those who already have the condition can benefit from adopting the following healthy lifestyle habits to aggressively address risk factors for the disease:
Certain food groups benefit health in general, and brain health in particular. These include:
• Fresh fruits and vegetables, such as green leafy vegetables, colorful fruits and berries, and carrots, which are high in brain-protective antioxidants;
• Whole grains, such as bread, cereal, pasta, and brown rice, which contain complex carbohydrates that provide the brain with glucose to increase energy and improve memory function;
• Lean protein from low-fat dairy foods, nuts, seeds, fish, and beans, and occasional servings of eggs, poultry, and lean meats to help keep your mind alert.
• Healthy fats, such as those found in canola and olive oils, which help lower levels of LDL (“bad”) cholesterol; polyunsaturated oils, such as those derived from corn and sunflower seeds, which help the body absorb vitamins, provide energy and heighten alertness; and omega-3 fatty acids, which are found in cold-water fish, as well as in flaxseed and dark-green leafy vegetables, which appear to play a key role in cognitive health and functioning and may reduce the risk of mild cognitive impairment or AD.
Caring for your brain requires not only adding nutritious foods to your diet, but avoiding these unhealthy foods as well.
• Trans fats (hydrogenated or partially hydrogenated oils) found in many commercially prepared fried foods, processed foods, and snack foods; • Simple carbohydrates, such as processed white rice and flour, sweets, and refined sugars;
• Sugar-laden soft drinks. Quench your thirst instead with about eight glasses of water daily to avoid dehydration that can negatively affect cognition.
• Watch your waistline: A high body mass index (BMI, a ratio of height to weight used to measure obesity) is associated with poorer mental skills in older adults. In general, individuals with a BMI of 25 up to 30 are considered overweight, and those with a BMI of 30 and over are considered obese. In one study, overweight and obese participants had smaller, older-looking brains than people of normal weight, of “severe brain degeneration.”
The brain regions affected by obesity are the same as those involved in AD, but the good news is that some studies have found a connection between losing weight and improved memory.
Exercise
A sedentary lifestyle increases risk for cognitive decline, as well as conditions linked to Alzheimer’s, such as diabetes, high blood pressure, and obesity. Inactivity may also significantly increase risk for vascular dementia (VaD), another common form of dementia. Regular exercise is one of the most important strategies available to reduce risk for dementia, and a large body of evidence supports its benefits for the brain. A good aerobic workout increases the flow of oxygen-rich blood to areas of the brain responsible for learning and memory and increases levels of brain-derived neurotrophic factor (BDNF), a chemical that protects neurons and strengthens synapses in the brain.
Forms of exercise that work several different areas of the brain at once–such as the eye-hand coordination, decision-making, and rapid information processing called for in playing ping-pong or tennis–have been linked to enlargement of a part of the brain that typically shrinks in patients with dementia. The earlier you start getting fit, the better. If you’ve been inactive for a while, ask your doctor to suggest an exercise program that’s safe for you. Aim for at least 30 minutes of aerobic exercise at least five days a week. Include exercises to improve muscle strength, balance, and coordination. Vary your activities to stay engaged and avoid boredom. Remember that even household chores and gardening count as exercise.
Break bad habits
Studies suggest that changing such habits as smoking and heavy drinking can be beneficial in warding off Alzeihmers.
• Smoking is detrimental to physical health, and the deleterious effects of smoking on the brain include neuron damage in the midbrain and hippocampus. If you smoke, talk to your doctor about smoking-cessation aids and other ways to help you quit.
• Chronic heavy drinking has been linked to brain atrophy, impaired memory and learning, and disrupted communication between brain cells. Excessive alcohol consumption is of special concern in older adults, because with advancing age, people become increasingly vulnerable to the effects of alcohol. In an older brain, alcohol may accelerate normal aging, aggravating symptoms of cognitive decline and early dementia. If you drink, do so in moderation. Women should have no more than one glass of alcohol a day. Men should limit themselves to one or two glasses (confirm this amount with your doctor). Avoid illicit drug use entirely.
Manage your medications
A number of medications commonly prescribed to older adults have unwanted cognitive side effects. Because your sensitivity to the effects of drugs increases with age and medications tend to linger longer in your system, side effects can show up at lower doses than they did when you were younger. Any decrease in cognitive function that occurs soon after you start taking a new drug or change the dosage suggests that medication may be the cause of the cognitive difficulty. It’s also advisable to review with your medical care provider regularly an updated list of your medications—including any over-the-counter drugs and natural medications they are taking. This type of patient-doctor consultation can help prevent unwanted side effects, dangerous interactions among various medications, and unnecessary over-medication that can lead to memory problems in older adults.
Although many drugs can impair memory, some of the most common examples of include:
• Benzodiazepine-like hypnotics used to treat anxiety, insomnia, and sleep disorders: zolpidem (Ambien);
• Antidepressants used to treat depression: venlafaxine (Effexor), fluoxetine (Prozac), and paroxetine (Paxil, Pexeva);
• Newer anticonvulsants used to treat epileptic seizures, bipolar disorder, and nerve pain: gabapentin (Neurontin), lamotrigine (Lamictal), levetiracetam (Keppra), pregabalin (Lyrica), and topiramate (Topamax)
Reduce stress
Although an occasional stressful situation doesn’t have lasting consequences for the brain, excessive or prolonged feelings of pressure, tension, and distress—with associated increases in levels of the stress hormone cortisol—can negatively affect the networks of dendrites that connect neurons with one another, reducing communication among brain cells.
High levels of stress slow the creation of new neurons to replace injured or dying cells, resulting in the gradual shrinkage of a key memory area called the hippocampus and higher risk for Alzheimer’s disease. Long-term stress also interferes with the proper functioning of neurotransmitters–chemicals responsible for transmitting messages from one brain cell to another–and impairs the functioning of the prefrontal cortex, the decision-making center of the brain responsible for short-term memory.
You can protect your brain from the harmful effects of stress and reduce your risk for memory problems by learning relaxation techniques to help lower breathing rate, blood pressure, oxygen consumption, and oxidative stress on cells. Stress-reducing relaxation techniques include deep-breathing exercises, yoga, tai chi, progressive relaxation, visualization, meditation, and relaxing activities such as listening to soothing music or taking a warm bath. If you are feeling overwhelmed by stress, consider seeking help from a mental health professional.
To get a better night’s sleep and bolster your memory, establish good sleep hygiene by adopting the following strategies:
• Go to bed at the same time each night and awaken at the same time each morning.
• Sleep in a cool, quiet, darkened room.
• Do something relaxing before bed, like reading a book or taking a bath.
• Avoid large meals or exercise within four hours of bedtime, and restrict liquids close to bedtime to avoid sleep interruptions for bathroom visits.
• Limit alcohol and avoid caffeine at least four to six hours before you go to bed.
Staying socially active.
Having close relationships and staying socially active requires paying attention to your surroundings, following a conversation, responding to the actions of others, and watching for verbal and non-verbal cues—all of which require a lot of brainpower. Research suggests that individuals who are least socially active experience a 75 percent greater rate of cognitive decline than those who are most socially active, even after other factors such as age, general health, and physical activity are considered. To keep your memory sharp, get out with friends as often as you can, and call, email, or Skype with friends and loved ones.
If you’re socially isolated, begin a campaign to win new friends.
Stay mentally active
A large body of evidence suggests that exercising your brain with stimulating and challenging activities, such as reading the newspaper, playing checkers, or taking dance lessons can keep you sharp and help prevent dementia. Activities that require concentration, use many senses at once, and involve new or unexpected experiences and approaches are especially stimulating to the brain.
Some research suggests that brain-stimulating activities help counteract the effects of aging by keeping the brain efficient and reducing the production of toxic beta-amyloid. Other studies suggest that mental activity may actually reshape the brain through the promotion of powerful growth hormones such as brain-derived neurotrophic factor (BDNF), which promotes the development of communication points between neurons, called synapses.
Protect your brain from injury
Traumatic brain injury (TBI), caused by a fall, blow to the head, or even violent jarring, can injure sensitive brain tissues in ways that might cause later declines in cognition. Symptoms of TBI vary depending on the area of the brain affected by the injury, and may not show up until hours, days, or even weeks later. Prompt medical treatment may help prevent further damage to vulnerable tissues.
Taking steps to avoid head injury is a wise precaution. Some common-sense suggestions include eliminating fall hazards in your home, using vehicle seat belts, wearing appropriate footwear, and wearing a helmet when engaging in activities with a risk of head injury, such as bike riding.
VII. HOW TO IMPROVE MEMORY
You can take steps to preserve your memory as you age. Try some of the suggestions in this chapter to organize information, cement it in your mind, and recall it more easily.
Learn Basic Memory Skills
These simple approaches will help make information easier to retain and recall:
• Concentrate. Focus on one memory task at a time.
• Make sure you understand the information you are trying to remember.
• Make an effort. To motivate yourself to remember, consider how the information will be useful to you.
• Use mnemonic strategies and other memory techniques. Rhymes, acronyms, or other forms are easier for your brain to encode and recall.
• Associate. Connect new bits of information with things you already know.
• Manage your memory. Break the information you want to remember into small chunks so that you don’t overload your memory. Take breaks during the process of remembering to give your brain a rest.
• Get organized. Keep frequently used belongings such as car keys in the same place, so you can find them readily. Use memory aids, such as calendars and automated medication dispensers. Make a weekly plan in which you note your goals, activities, appointments, and chores for each day of the week to help you stay on track without cluttering your mind with minutiae.
• Use cues and reminders. Put your empty medicine bottle by the door to remind yourself to refill your prescription. Use a timer to remember to turn off the oven.
Train Your Brain
Regularly engaging in training exercises that help you practice specific cognitive abilities (e.g., attention or processing speed) seem to protect against memory loss better than memory strategies alone. Examples of cognitive exercises you might try:
• Strengthen your powers of attention by concentrating on one subject or task for 10 minutes without letting your mind wander. The next day, increase your concentration time to 12 minutes. Play online brain-training games to boost your brain’s processing speed. Memorize your favorite poems, or learn to play a new piece on the piano.
• Boost information processing speed by playing online brain-training programs. Another option: examining a photograph you have not seen before for one minute. Then turn over the photo and jot down as many details from it as you can remember. As your processing speed improves, shorten the time you spend examining each new photo.
• Exercise your capacity to recall information by reading a medium-length article on any subject while making an effort to remember as many details as you can. Put the article aside and write or recite as much as you can of its contents. Then check the original article to see how you did. Make Information Stand Out To increase your ability to retain a memory, use one of the following imaginative techniques to endow it with unique elements or associations so that it stands apart from other information you may be exposed to at the same time:
• Take a snapshot: Create a mental “photograph”—a visual record of what you want to remember–noticing as many details as possible.
• Prepare a speech: Pretend you must describe or explain the information you want to remember to someone else.
• Sing it: Make up a song or jingle containing the information you’re trying to remember.
• Create a vivid mental image: For example, to remember the peanut butter, chicken, and olives on your grocery list, picture a chicken covered with peanut butter wearing a necklace of olives.
• Laughter is the Best Medicine, Shopping Cart Therapy, Rides in the Car And Solving Puzzles.
Mindfulness Meditation
Research suggests that the ability to pay attention—a key aspect of memory—declines with age. One excellent way to improve your ability to pay attention and remember is to practice mindfulness meditation. This form of meditation involves focusing your awareness on sensory stimuli in the present moment, while ignoring intrusive thoughts and inner chatter.
Research suggests that older individuals who meditate have better preserved cortical regions of the brain—regions responsible for attention, sensory processing, and integrating emotional and cognitive processes that normally thin with age. To meditate, follow these basic steps:
• Find a quiet place where you can meditate without being disturbed.
• Sit comfortably, close your eyes, and slow your breathing.
• Focus on your breathing, or on a simple word or syllable uttered as you exhale.
• Be aware of sensory perceptions, but remain detached.
• When your mind wanders, bring it gently back to your breathing or focus word.
• After 20 minutes or so, open your eyes and sit quietly for a moment, letting yourself gradually return to your normal state.
If you believe Noah’s flood verbatim, you believe that the world was repopulated through incest. Considering who survived the flood. One can be a believing Christian and not dismiss science. Pastor Taiwo Larry logic tells me there was more than one Noah. The world has too many species for one boat. And Noah and his family couldn’t have replenished the earth. That’s why it’s not logical. It’s only 1 story. It’s limited.
The flood story was “borrowed ” from the Epics of Gilgamesh which predate Christianity by a few thousand years.
Well before Noah. The vast majority of Archaeologists don’t accept the Great Flood fairy tale. You lie.
Why must you people lie for your god? Does it please him? Geez.
Are you sure it wasn’t the older Gilgamesh flood or the one Zeus the King of the gods created! It’s almost as if the story was plagiarized.
The story and note of Noah’s Ark doesn’t even originally originate in the Bible; it was previous civilizations that existed long before the 6000 years that the Bible claims. And if you really think the Earth is 6000 years old you’re a complete buffoon.
A Lot of the science or what we once knew of it has been proven wrong by technological advances as well as archeological discoveries.
The mountain was created when plates drifted and crashed. India. Into China. Pushing the sea floor upwards. Bring the bottom of the sea up. Creating the mountain. FYI Himalayas was formed during the early Tertiary period following the K-T impact event when the Indian Subcontinent collided with Eurasian Plate.
The Himalayan mountain range and Tibetan plateau have formed as a result of the collision between the Indian Plate and Eurasian Plate which began 50 million years ago and continues today. – Read Genesis 8.
And amazingly the Mariana Trench is deeper than Everest is tall!
Except it wasn’t. the ROCKS at the top of Mt. Everest was below the sea, not the mountain.
The rocks were pushed to the top of the mountain by tectonic plate collision that essentially ‘stacked’ large chunks of rocks on top of each other and formed a mountain. Does this have anything to do with Genesis 1 in the Bible?
The Bible recorded that the face of the earth was covered with water and caused the water to make way for land.
The correct info of this earth lies in the hands of the ALL POWERFUL CREATOR. Not scientific
Which proves the Bible viewpoint that says the earth was actually full of water before Jehovah commanded land to surface.
Genesis 1:2, which states: “Now the earth was formless and void, and darkness was over the surface of the deep. And the Spirit of God was hovering over the surface of the waters.” ¹ Additionally, Genesis 1:10 says: “And God called the dry land Earth; and the gathering together of the waters called the Seas: and God saw that it was good.” ²
It’s a demonstration of how the Earth’s crust is in constant movement and has been for billions of years. The crust has split up into ‘plates’ as a result of this movement and the plates grind slowly in directions that in some regions bring plates into ‘conflict’. Everest is part of the Himalayan mountains of India, which has been slowly drifting north into the Eurasian plate for 100 million years, forcing up the rocks which are at the leading edge and were originally below sea level, hence those limestone rocks and marine fossils. Google it : it’s fascinating.
Makes the accuracy of the Bible stating the beginning of all things!.
Genesis 1:9 And God said, Let the waters under the heaven be gathered together unto one place, and let the dry land appear: and it was so.
10 And God called the dry land Earth; and the gathering together of the waters called the Seas: and God saw that it was good.
Me: The bible is right in every way!!.
The Bible remains the most accurate BOOK no matter how the enemy (Satan) and his agents in the world have tried to tamper with it, it still remains “the accurate” but its inspiration remains of the Holy Spirit. If you don’t get this??
PRAY FOR THE HOLY SPIRIT TO HELP YOU WITH THE PUREST OF UNDERSTANDING. FEAR GOD. There was no earth until He spoke!
May the word of God minister life into your living; for new things to begin to happen in your life as you “believe” in Jesus Mighty. Amen
Genesis 1:1-2,9-10 KJV
In the beginning God created heaven and the earth. [2] And the earth was without form, and void; and darkness was upon the face of the deep. And the Spirit of God moved upon the face of the waters. [9] And God said, Let the waters under heaven be gathered together unto one place, and let the dry land appear: and it was so. [10] And God called the dry land Earth; and the gathering together of the waters called the Seas: and God saw that it was good.
Basically the whole earth was filled with water thus even this mountain was submerged
For those referencing Noah’s flood, please note that the flood lasted 40 days and nights. This duration was not sufficient to change rock structures.
According to the Genesis 1:9 account, the Earth was created from a mass of deep waters that receded to reveal land.
This could explain why some terrestrial rocks are structurally similar to marine rocks, as they share a common origin according to the biblical narrative.
u.S.Psalms 104:5-9 NKJV
[5] You who laid the foundations of the earth, So that it should not be moved forever, [6] You covered it with the deep as with a garment; The waters stood above the mountains. [7] At Your rebuke they fled; At the voice of Your thunder they hastened away. [8] They went up over the mountains; They went down into the valleys, To the place which You founded for them. [9] You have set a boundary that they may not pass over, That they may not return to cover the earth.
What so many bible followers fail to understand is that in the Vedas, there is also a flood story that is talked about where the world is inundated. So this proves the Vedas as well
Genesis 6. The world is still catching up with what God told us many centuries ago
These rocks, deposited in an ancient Tethyan Ocean were thrust and uplifted into their present commanding position when India collided with the Asian continent some 55 million years ago. Most people know this from an early age, so shame on your country’s educational system or shame on you for not paying attention in school. Shame on you for not learning to use the internet properly. Does not prove the Bible.
You’re ignoring plate tectonics and a process called uplift that happens when two plates, the Indian and Eurasian, push against each other. The Indian plate subducted under the Eurasian plate, causing the continental crust to crumple and get pushed up. This would cause Continental crust that may have been covered with ocean at the time to be uplifted many many kilometers.
That means that the limestone, formed from most likely the calcium carbonate shells of Plankton as they died and settled, to be thrusted upwards and now reside at the top of a mountain. So, this does not prove that the world was flooded because there is another logical explanation that is very well supported by many pieces of evidence and is replicated in many other areas of the world where you have mountain ranges formed by the same process.
Education. It’s worth something.
Of course it was. It was called the great flood!
For 40 days and nights God flooded the World killing everything. He found that all the people of the Earth were EVIL. JUST LIKE ALL THE EVIL IN OUR WORLD! Now he PROMISED that he would never FLOOD the World again. THAT’S WHAT THE RAINBOW MEANS. NOT FOR THE lbgq+- Whatever it’s called, it’s CALLED SIN IN GOD’S EYES.
That old Bible is going to be right every time, and I have no trouble believing it.
Gen 6:17 And, behold, I, even I, do bring a flood of waters upon the earth, to destroy all flesh, wherein is the breath of life, from under heaven; and every thing that is in the earth shall die.
IT COLLABORATE THE HOLY SCRIPTURES IN GENESIS Chapter 1 vs 2:
Now the earth was formless and empty, darkness was over the surface of the deep, and the Spirit of God was hovering OVER THE WATERS. MAY GOD ALMIGHTY (not the African pastors god) BE PRAISED.
This is to that godswill aguinem guy that keeps erasing my reply to his comment, which idk why he keeps doing that.
Probably because he doesn’t want to hear what someone who has seen the other side before. But ya I was baptized. And I had a suicide attempt 11 years ago that left me brain dead for 2 days and with 8 strokes in all parts of my brain. And I still to this day remember parts of what I had “seen” on the other side. And news flash there was no bright golden light or anything like that, it was just blackness. But I will say that it was peaceful. I just will never go back to something that is so wrong and has ruined so many lives it’s almost impossible to comprehend.
Religion is just a pacifier for the masses and to make people have peace for when they are in times of distress or at the end of their lives. Which usually I’d be like well that’s good then. But if you actually look back at how many people have died as a direct result of religion because of holy wars.
You can’t sit back and say that religion is peaceful and harmless. You just can’t, Cause if it was there would be no holy wars. Whether you think of the crusades or the sacred wars and many other “holy” wars, religions are the biggest and longest scams in the world. And that was the first time I have died. The 2nd was a seizure when I was 21 but I wasn’t brain dead at that time.
God said, let the water under the sky be gathered Into a single basin , so that the dry land may appear, and so it happened, GOD called the dry land, the earth, and the basin of the water He called, the sea. Genesis 1 : 9 – 10
Read the book worlds in collision. A very amazing book. From Emanuel veilkowski. Paul segan. Einstein. Steven Hawking And others. Read this amazing book. And praised it….Revelation 16:20-And every island fled away, and the mountains were not found. As the sea level rises. Just not as much as what’s been basically propagandized. Most of that missing water went into earth’s mantle over millions of years and basically cooled down the earth enough to allow life to flourish.
But what didn’t find its way into the Earth’s mantle that also isn’t in the oceans is whatever giant ice caps are still on land. Ice caps already in the oceans don’t displace the oceans when they melt but ice caps on land will certainly raise the sea when they melt because all the water will eventually find its way back to the ocean just as all water eventually does in earth’s water cycle… But that’s millions of years worth of activity so it shouldn’t be anything to worry about.
In the Bible, when God broke up the depths of the Earth, the ripple effect pushed the landmasses back like someone pushing a rug up against the wall; that’s why most of the mountains of the world are somewhere near a body or stream of water.
Geologists are starting to accept now, mountains were formed along with the world faults and the Grand Canyon, and lastly, the craters of the world were due to the great flood.
“In the six hundredth year of Noah ‘s life, in the second month, on the seventeenth day of the month, on that day all the fountains of the great deep burst forth, and the windows of the heavens were opened.” Genesis 7:11
If all the glaciers melt, water will go up about 70-80 meters. That’s not even close to what’s needed to cover the Himalayas.
Yes, they erupted about 60 millions years ago when India collided with the rest of Asia. Which explains differences in plant and animal diversity there.
There was never global food. There were local floods, though, which gave origin many stories, as a myth of global flood was before Judaism borrowed it.
The Himalayas were formed from the materials that were originally part of the Tethys Sea. Here’s a more detailed explanation:
1. **Sediment Accumulation**: During the existence of the Tethys Sea, a vast amount of sediment from rivers draining into the sea accumulated on its floor. These sediments included mud, sand, and the remains of marine organisms.
2. **Plate Collision**: The Indian Plate moved northward and collided with the Eurasian Plate. This collision caused the oceanic crust of the Tethys Sea to be subducted beneath the Eurasian Plate, while the accumulated sediments were caught in the collision zone.
3. **Uplift and Folding**: The immense pressure from the collision caused the sediments and oceanic crust to be uplifted and folded, forming the mountain range we now know as the Himalayas. This process began around 50 to 60 million years ago and continues today.
4. **Geological Composition**: The Himalayas consist of various rock types, including:
– **Sedimentary Rocks**: These include limestone, sandstone, and shale, which were originally deposited in the Tethys Sea.
– **Metamorphic Rocks**: The intense pressure and heat from the collision transformed some of the sedimentary rocks into metamorphic rocks, such as schist and gneiss.
– **Igneous Rocks**: There are also igneous rocks that formed from volcanic activity related to the tectonic processes.
5. **Marine Fossils**: Fossils of marine organisms, such as ammonites and other marine life, are found in the sedimentary rocks of the Himalayas. These fossils provide direct evidence that the rocks were once part of the Tethys Sea floor.
In summary, the Himalayas are composed largely of materials that originated in the Tethys Sea. The tectonic collision between the Indian and Eurasian plates uplifted and transformed these materials, creating the towering mountain range.
Scientists say that if Mount Everest was placed under the Philippine Deep (or was it the Marianas Trench), it would be under the water even at its highest peak, with still much room to spare. This is quite accurate for they have on record their respective depth and height.
So scientists believe at one time all continents were fused together and. Over time have separated from plates shifting.then the axis of the planet have shifted 3 times.yes this earth has changed form constantly over the millennials, and some people now telling you climate change is a threat.wow,you need to wake up fast
Fact check: the summit of Mt Everest is made of marine limestone
COPILOT Yes, the summit of Mount Everest is indeed made of marine limestone. This fact has been established through geological studies of the mountain’s composition. The marine limestone found at the summit of Mount Everest dates back to around 450 million years ago, during the Ordovician period.
References
For a more detailed explanation and confirmation, you can refer to:
Geological surveys and academic papers on the composition of the Himalayas.
In summary, the summit of Mount Everest is indeed composed of marine limestone, a testament to the dynamic geological processes that shape our planet.
The continents were one and the animals were everywhere, because of the flood the tectonic plate was broken up, mountains and, weather patterns came to be, the continent was pulled apart and animals settled into different locations all because of that great and terrible flood that changed the geology of the planet.
I only have a rudimentary understanding of mountains which are raised over millennia as plates slide under each other. From memory the Himalayas are at the edge of a plate? Stands to reason this mountain was once much lower than it is now. So perhaps the sea level was as high as being suggested.
It’s not far from flipping!
No escape from the velocity of the water from mountains and oceans colliding. It could be very tragic to all mankind. Global Warming is playing a part in how quick this happens.
Every 10-12 thousand years or so.
No! Each unfreezing, after each subsequent ice age, of fresh and mineralized saline water, revealed the living residues from each type of aquatic environment, after the thawing of the ice, as the higher landscapes, deposit its ice-covering into the depressions, thus the continuous rising of its encompassing Oceans and lakes, even onto today, claiming low-lying shorelines, also claiming low-lying islands. This repetitious process precedes the natural repetitive cycles of Solar, Nocturnal, and Ice ages. Our Earth is full of evidence to support the occurrences of these ages, in fossilized remains, embedded in deep stratification of our Earth e.g. Coal and crude oil are aged sediments of various materials, from cycles of ages past.
To be pedantic, the Indian subcontinent is pushing under the Eurasian plate, pushing former seabed up into the air.
Everest is the highest above sea level, but not the highest point from the center of the Earth. The Earth isn’t a perfect sphere. It’s slightly oval shaped. The distance around the equator from where you start and finish at the same spot is 24,901 miles. The distance around the Earth’s poles is 24,860 miles. That’s a difference of 41 miles. Mount Chimborazo is only one degree from the equator. Everest is 28 degrees from the equator. Chimborazo gets a boost because it’s practically at the equator. Measuring by sea level isn’t exactly the best way to measure the height of mountains. It’s just something that was decided the right way, but it’s not. Chimborazo is just sitting on higher ground.
Many scholars believe that the flood myth was added to Tablet XI in the “standard version” of the Gilgamesh Epic by an editor who used the flood story from the Epic of Atra-Hasis1. In the Gilgamesh Epic, the story of the flood is related as part of the tale of Gilgamesh’s quest for immortality2.
Utnapishtim tells his descendent, Gilgamesh, the story of the flood in order to tell Gilgamesh how he, Utnapishtim, became immortal; in so doing, he shows Gilgamesh that he cannot become immortal in the same way3.
The Epic of Gilgamesh conveys several moral lessons.
Here are a few key takeaways:
Mortality and Immortality: The story explores the quest for immortality. Gilgamesh, initially obsessed with avoiding death, learns that true fulfillment lies in accepting mortality and living a meaningful life.
Friendship and Companionship: The bond between Gilgamesh and Enkidu highlights the importance of friendship. Their adventures together demonstrate the value of companionship, loyalty, and shared experiences.
Responsibility and Leadership: As a king, Gilgamesh learns that leadership involves caring for his people and ensuring their well-being. His transformation from a selfish ruler to a wise leader reflects this lesson.
Respecting the Divine Order: The gods play a significant role in the epic. Gilgamesh’s defiance of divine authority leads to tragedy, emphasizing the need to respect cosmic order and divine will.
Appreciating the Present: The story encourages us to appreciate life’s fleeting moments. Gilgamesh’s realization that he cannot escape death prompts him to cherish the present.
Remember, interpretations may vary, these themes resonate across cultures and time. 🌟
How does the Epic of Gilgamesh compare to other epic tales?
Certainly! The Epic of Gilgamesh stands out as one of the oldest tragic epics, dating back to around 1,800 B.C.E. It follows the adventures of the semi-divine King Gilgamesh, who seeks eternal life and battles mythical beasts. Here’s how it compares to other epic tales:
Noah’s Ark (Genesis):
Similarities: Both narratives feature a catastrophic flood, a chosen survivor (Noah or Utanapishtim), and the release of birds to find dry land.
Differences: Gilgamesh’s flood is more vivid and violent, involving multiple gods, while Genesis focuses on monotheism and a less detailed storm.
Hesiod’s Theogony:
Difference: Gilgamesh follows a single character’s journey, whereas Theogony involves several characters and their origins2.
Cosmic Worldviews:
Gilgamesh and Genesis reflect different cultural values and cosmic perspectives. They’re in dialogue with each other, shaping ancient Mesopotamia and Hebrew worldviews.
Other Parallels:
Sage advice from Gilgamesh appears in Ecclesiastes (Hebrew Bible), emphasizing shared wisdom across cultures.
In summary, these epics offer unique insights into humanity’s quest for meaning, mortality, and divine order. 🌟
Throughout my lifetime (and probably yours, too), I have personally experienced and heard about others experiencing all kinds of natural disasters and worldwide events. For example, since I am old enough to remember, I have known of earthquakes, hurricanes, volcanoes, and tsunamis that have devastated lands, destroyed homes, and taken people’s lives. Wildfires have charred thousands of acres of woods and anything else in their path. Solar eclipses, comets, and solar flares have caught the attention of billions of people, causing them to look up in wonder.
On top of all of those natural events, humans have been the cause or at least catalyst for wars and riots claiming the lives of countless people, viruses affecting whole countries, and violent regimes causing the genocide of whole races of people.
A natural disaster is, well, anything that’s not natural, but really these catastrophes are nothing new to earth’s and humanity’s history. There was a global cooling event in the 17th century called Europe’s Little Ice Age, but what caused it? For around a 70 year period (from 1645 until 1714), early astronomers reported almost zero sunspot activity. The number of sunspots, which are cooler areas on the sun that appear dark against the brighter surroundings, dropped roughly a thousand fold. And then there’s the Little Ice Age which began around 1300 A.D. and ended up lasting for several hundred years.
The result was ruined crops, widespread poverty, and death. The world endured much colder than normal winters and much cooler summers than normal for centuries, at least in the Northern Hemisphere, but this could have been caused in part, by particulates spewed into the atmosphere by volcanoes, combined with fluctuations in the sun’s output. The point is we have always experienced natural disasters in the history of mankind, but is it getting worse?
However, some of that data may be skewed because we’ve had more widespread media coverage worldwide, and who doesn’t seem to have a cell phone these days to capture the next natural disaster? I do not believe that all these increasing catastrophes are a coincidence. Something seems to be going on with the earth, but is there a spiritual cause at the root of all this? There may be. Read on.
Vomited Out of the Land
There are actually Old Testament Scriptures that talk about the land vomiting its inhabitants out of the land, due to the heinous and grievous sins that the people were doing. That was primarily idolatry, but when it came to a nation sacrificing their own children in the fire to a pagan God (actually satanic demon), God said, “It is enough!” The land of Canaan was defiled by the children of Canaan and so it was said that the land vomited them out (Lev 18:21). Vomiting a people out could be by means of a nation invading them (Israel did Canaan), people moving out as asylum seekers, refugees, slaves, prisoners (Israel would later be taken captive by Babylon), etc.
God Judges the Nations
The Bible shows many examples of where a nation was “vomited out,” either by another nation or power or through natural disasters (Sodom and Gomorrah), but however God chooses to do this, there is a point in time when the land will vomit out its inhabitants (Lev 18:24-25). How it happens is when “the land became unclean, so that I punished its iniquity, and the land vomited out its inhabitants” (Lev 18:25), so God can vomit (expel) out any nation that turns its back on God, and reaches a such a sinful state that it’s stench reaches up to heaven.
This same thing happened in Noah’s day (Gen 6) when God said it is enough. He has done this before and He can do it again, so the question is, “What is the tipping point when God moves in judgment against a nation, particularly a nation that’s murdered multiple millions of babies through abortion like America has?” And what of the other nations around the world living contrary to God’s Word? If God did not spare His own Son, what makes us think He’ll spare any nation that kills its young, even in the womb (Rom 8:32)?
Conclusion
With all of the world’s problems and natural disasters, there’s not much certainty about the future for unbelievers, and if you have not yet trusted in Christ, I hate to tell you this, but you have absolutely no access to God nor can you seek help from Jesus Christ when disaster strikes. Until God brings you to repentance and you put your trust in Christ, you are all alone in passing through this life, but it is never too late to turn to God. Make today your day of salvation instead of having your heart hardened by rejecting Christ over and over (2 Cor 6:2).
That’s a dangerous place to be, dear reader. Until you have put your trust in Christ, you will have to bear every anxiety and every burden yourself, so please, I plead with you, why not trust in the Savior today and let Him carry what you cannot carry yourself? He is there right now…waiting for you. He holds the future secure in His hand. That’s something we can take comfort in. Even if the world looks like it’s out of control, we know God is not (Rom 8:28).
Resource – Scripture quotations are from The Holy Bible, English Standard Version® (ESV®), Crossway Bibles. (2007). ESV: Study Bible: English standard version. Wheaton, Ill: Crossway Bibles. Used by permission. All rights reserved.
A vast swath of lands from eastern Nebraska and South Dakota to Iowa and Minnesota has been under siege from flooding from torrential rains since last week, while also experiencing a scorching heat wave.
One 10-foot-high meteotsunami in Lake Michigan killed five people and endangered 27 others on July 13, 1938 in Holland.
The wave reportedly came out of nowhere on a calm afternoon. Members of the Coast Guard tried to warn swimmers not to go in the water, but the wave’s “sudden” undertow pulled swimmers into rough waters, while the wave threw people off of piers.
“It looked as if the lake took a deep breath and all at once the calm was broken,” Coast Guard member Robert Bush told the Holland City News the next day. “The surf rolled on the beaches, and within 10 minutes the breakwaters were awash. After the calm there was not much wind, but it seemed that there must have been terribly heavy squall further out in Lake Michigan.”
The term was coined in reports from the UNEP Indian Ocean Experiment (INDOEX). It was found to originate mostly due to farmers burning stubble in Punjab and to lesser extent Haryana and Uttar Pradesh. The debilitating air quality in Delhi is also due to the stubble burning in Punjab.[3]
Asian brown cloud, a large atmospheric brown cloud that occurs annually from about November through May over eastern China and southern Asia. The Asian brown cloud is caused by large amounts of aerosols (such as soot and dust) produced in the combustion of fossil fuels and biomass across the region.
While these predictions may seem outlandish, they serve as fascinating examples of human imagination and our enduring fascination with the end of days. Fortunately, none of them have come true! 😅🌎
The prophecies contained in the Book of Revelation are key end time revelations which we must prepare ourselves for, as the end time is happening now.
The prophecies of the Book of Revelation are among the most important parts of the Bible, and understanding these words is a crucial component of understanding how the end times will unfold. Most importantly, the end time revelations that are uncovered in Revelation show us that the end time is not a one-time event that destroys the planet in one fell swoop. A set series of events have been prophesied, which we can anticipate to occur imminently as we now have a clear picture of the end times.
The Seven Seals, the Seven Trumpets, and the Seven Vials
One of the most distinguishing end time revelations that has been revealed to us through the Book of Revelation is that many different events will be occurring over a relatively short period of time. The Seven Seals described in Revelation is the longest story of the end times – a series of disastrous events occurring with major impact on the world stage. The text also helps to understand when the opening of the seals will happen in our time, with the Great Tribulation happening between the opening of the sixth and seventh seals.
The Seven Trumpets sounded well when the seals were opened – but what many people do not realize is that five of the seven trumpets have already sounded. This is one of the biggest signs that the end time is upon us, especially with the Sixth Trumpet War (Revelation 9:13-21) that will soon take place in the Middle East where there is currently so much turmoil.
The end time revelations have one more crucial part that explains what the signs of the end times are, including when they will take place. The Final Seven Years will begin with a time of relative calm – three and a half years when we will see an interim peace in the Middle East over the Temple Mount by the people of Israel and Palestine.
However, during the second half of this 84-month time period, Revelation explains that things will quickly get worse. The Antichrist will take his place as the leader of the world, ushering in the Great Tribulation (Revelation 12:12) and many of the disasters referenced by the Seven Seals. We are also given a warning about the Mark of the Beast and the Antichrist’s ploy in creating allegiance to a one-world government.
Understanding More of the End Times
While these end time revelations are filled with death and destruction, the Bible also gives us hope in the name of Jesus Christ – the prophecies reveal that all of these disasters will end with the restoration of the Kingdom of God.
The end times are a complex subject, and it’s very easy to be deceived about their meaning even if you study the Bible with the best of intentions. Endtime Ministries has developed materials that explain the Book of Revelation so that each prophecy makes sense in the context of today’s society. The Revelation Commentary DVD series – Search Videos (bing.com) and its accompanying study manual can help you understand the truth of the Bible’s end time revelations and what they will mean for you.
This Hospice Nurse Is Answering Taboo Questions About Death And Dying, And I Learned So Much, Recently, we wrote about what the actively dying phase looks like, which occurs during the last phase of life. This was thanks to the help of Hospice Nurse Julie, aka @hospicenursejulie, who educates about death and dying on TikTok.
Julie, whose viral video about the actively dying phase now has almost 9 million views on TikTok, taught us about symptoms that may appear scary but are entirely normal — like the death rattle, the “rally,” end-of-life visioning, and “fish-out-of-water” breathing.
Julie wants to alleviate some of that fear around death and dying – she says that by educating ourselves about the final stages of life, we can better be there for our loved ones.
From the practical (like does it hurt?), to the taboo (do our bodily fluids really just release?), to the personal (like how can I deal with my death anxiety?) — here are all your questions Hospice Nurse Julie answered about death and dying:
1.”What does the actively dying phase feel like to the dying person? Do we know?”
Hospice Nurse Julie: The answer is we don’t know, technically. We use non-verbal pain scales to assess if the person is experiencing discomfort or pain. It’s pretty easy to see that in a dying body, if someone is comfortable or not comfortable. I do believe the person in the actively dying phase is fully unconscious so they’re not consciously in their body wondering what’s going on. I believe we can tell that because of the nonverbal cues the person is showing us.
Hospice Nurse Julie: So, I always like to say that dying itself does not hurt, especially if you’re dying a natural death, meaning like from a disease, but you’re allowing the natural progression to take over. That does not necessarily hurt, but the disease and its symptoms can cause pain. The actual act of dying — likely not. But the disease you’re dying from can cause symptoms that make you hurt, hence why we have, you know, doctors and nurses who can help with those symptoms so you can have an as peaceful as possible death.
4.”What happens with a pacemaker or defibrillator during the final minutes of death?”
Hospice Nurse Julie: A pacemaker is totally fine to continue to stay on during the dying process. It interacts with the electrical system in the heart. So, it will not continue to pace someone if the heart is no longer beating. So, that is not an issue; that can stay on. A defibrillator shocks a heart if it goes into dysrhythmia (an irregular heartbeat).
[Dysrhythmias are] a natural process of the death and dying process, and we shouldn’t worry about them. But the defibrillator should be turned off because if the person does go into an irregular rhythm during the dying phase, that person could be shocked, and being shocked is uncomfortable. So, just to be clear, it’s normal for the heart to go into irregular rhythms at the end of life.
5.”Do you lose control of your bodily fluids immediately?”
Hospice Nurse Julie: Not everyone at the end of life will lose control of their body fluids. It’s not like everyone will suddenly urinate and defecate because they have died. However, I would say at the end of life in the actively dying phase, everyone will be incontinent. So you will need someone to change you and care for you if you do die the natural, gradual way. Not everyone does — if you die, suddenly, that likely won’t happen. But if you’re dying a gradual, slow, peaceful, comfortable death, you do get to a place where you are unconscious, and someone has to change you because you still are urinating and having bowel movements. Maybe not as often as you normally would, but you still have them.
However, when someone dies, I think there is a little bit of a misconception that the second they die, they urinate and defecate. That’s just not true. They can at times, and that’s because all of the sphincters in our bodies, which keep fluids and waste in until it’s ready, will loosen and relax and then let go of bodily fluids, hence why people can have fluid come out of their mouth. They can have a bowel movement; they can urinate. That can happen immediately upon death, but it doesn’t always happen. It just depends.
6.”My mom has Alzheimer’s and doesn’t know who anyone is. Will she recognize those at her bedside at the last stage of dying?”
Hospice Nurse Julie: I would say no. Usually not. Every once in a while, and I’m sure this person has already noticed this, they’ll have really good days where suddenly they do remember their children, and they do remember things. So they could have intermittent phases in days and moments where they do recognize people.
But at the end of the day, Alzheimer’s is a progressive disease, and usually the last stage of dying, the person is nonverbal, bedbound, and not recognizing anyone. And even if they did, they can’t verbally say they are recognizing people. But really, I would say the last phases of Alzheimer’s are usually the most peaceful.
For years, people with Alzheimer’s have confusion, paranoia, and agitation because they’re very confused. You know, a lot of issues, and that can last for a very long time and be very hard. The last phases of life for someone with dementia or Alzheimer’s are usually pretty docile because they are sleeping 22 hours a day.
7.”The thing that broke my heart the most was, a few days before my uncle passed away in his late 80s, he started to cry and admitted he was scared. And I had no idea how to respond, so I just held his hand. What are some ways I can 1) respond to this or soothe a scared loved one, and 2) deal with my own fear and anxiety of mortality?”
Hospice Nurse Julie: This is a great question. Okay. So, number one, this person did the right thing. A lot of times, we feel like we have to say something to make the person feel better. Generally speaking, allowing someone to say their fears, and either just being silent and holding their hand and allowing them to have that and not try to push it away, like ‘No, no, no, no, no, don’t be afraid.
Don’t be afraid,’ it’s better. From my experience, allow that [fear] to happen, hold their hand, and be there with them, and maybe even answer truthfully. Whatever the truth is for them, right? ‘I’m afraid too. I can see how you’re afraid. And I’m so sorry. I feel afraid to.’ Or what I usually say, if this is helpful, I normalize how normal it is for people to feel afraid.
Hospice Nurse Julie (cont.): And then how can we deal with our own fears, right, our own fear? Again, it’s the same thing. It’s through talking about it. It’s through saying, ‘I’m afraid, I’m afraid to die, I don’t want to die, I’m afraid of it.’ That alone. Awareness around the fear can really help loosen the grip.
I’ve also heard many people who have death anxiety tell me that watching, learning, and educating themselves about how the body works during the dying process has helped alleviate a lot of their anxiety. I think education can help decrease fear and truly understand and contemplate our mortality — knowing it’s going to happen, knowing it’s normal to fear that, and soothing ourselves in the process. I think it’s when we deny the fear, deny thinking about it, not looking at it, is when the fear increases. I think fear decreases when we do look at that fear, when we do accept the fear, and when we do learn about what we’re actually fearing.
I hope that helps. I love that question.
8.”I have 200 medical problems. No exaggeration. I usually have a healthy emotional attitude about it all but sometimes it’s overwhelming. Will the doctors tell me when they think I’m nearing my time?”
Hospice Nurse Julie: You know, it depends on the doctor. I would say, in general, you be your own advocate. Talk openly about how you’re feeling, about your health issues, and about how you want to know what to expect with all of your doctors.
So, with all of your doctors, since you probably have several doctors you’re working with, you need to be open with them about how you want to prepare for the end of your life, even if they say it’s far off. ‘Oh, you don’t need to do that right now. ‘
No, I want to do it right now. I want to know. You have seen this type of disease over and over again. How do you normally see it progressing? What can I expect? And please, I’m asking you to be honest with me when you think I’m coming to a place where you’ve done all you can do. I would like you to have an open dialogue with me.
9.”I have incurable cancer and have felt/been very close to dying on several occasions. Medical science has kept me alive thus far. There’s a lot of advice and information about what happens when an older person dies, so my question is, what differences might there be when it’s a younger person? I’m still in my 20s and don’t expect to live to see 40.”
Hospice Nurse Julie: So, great question. I’ve seen many people die young because of hospice. People always think that people in hospice are old, and that’s just not true. I will say there’s usually a lot more terminal agitation at the end of life for someone younger because of the existential — they’re too young, right?
Hospice Nurse Julie (cont.): But I will say, because this person is asking this question already, I feel like there probably will be less angst. People, even when they’re young, who have come to terms and accept that they’re dying — which I’m not saying is easy or even necessary to do, I get if you’re like, ‘No, I’m not going to ever accept that’ — but people who do tend to let go a little easier at the end.
Now, how can you work on that? I think this is exactly how it works: by asking questions. Knowing and thinking about your end of life, how you want it to look, trying to really contemplate the fact that it’s actually going to happen. And because of that, how do you want to spend the rest of your time here? In doing that, you can help get yourself to somewhat of an acceptance of a knowledge and a belief, knowing that you’re going to die.
So, then you can change the way you’re living – if you want to change the way you’re living — to help you feel less like you didn’t do the things you wanted to do or spend the time the way you want to spend it. But I feel like the person asking this question is already kind of a step ahead because they’re already thinking about it, which is going to help tremendously.
Julie shares the lessons she’s learned in her 15 years as an RN in the ICU and hospice, answers more of your questions, and destigmatizes conversations around death and dying.
Dr. Carl O. Helvie, AUGUST 13, 1932 – DECEMBER 3, 2019
NOTE: On Carl’s Death Bed, I made a promise to Carl I would keep his journey going.
Carl O helvie – Search Videos (bing.com) Professor, nurse, author, radio host, researcher and holistic health advocate. Born August 13, 1932, in Gouverneur, New York, his career spanned more than 60 years as a nurse practitioner, educator, author, and researcher.
Carl was a registered nurse and Professor Emeritus of Nursing at Old Dominion University where he taught nursing for nearly 30 years. He was also known for his development and implementation of the Helvie Energy Theory of Nursing and Health, the publication of this 1998 textbook, Advanced Practice Nursing in the Community, and his work with the local homeless.
Carl received a doctorate in public health from Johns Hopkins University, a master’s in public health from Johns Hopkins, a master’s in public health nursing and also focusing on wellness from the University of California, a B.S. in nursing from New York University and undertook post-doctoral study in the Divinity school at Duke University.
Carl was preceded in death by his father, Charles Helvie, his mother, Georgia White, stepfather David White and four siblings. He is survived by two sisters.
“I was saved from lung cancer in 1974 for a reason;
The difference between a bureaucratic administrator and a people-oriented leader can be seen in the results. The bureaucracy provides marginalized service erring towards sustaining dysfunctional systems at the expense of the people that are supposed to be served. The top administrators will be well paid in spite of the fact that (1) the work environment is stressful and inefficient, and (2) the clients receive compromised or useless goods and services.
The people-oriented leader will constantly challenge bureaucracy, cutting fat, eliminating redundancy, and fostering a culture of community and compassion by putting the needs of people above rigid guidelines, self-serving agendas, and grandfathered parasitic systems.
As a solution-oriented thinker, Carl O. Helvie is a bureaucrat’s nightmare; when necessary, he does not hesitate to bypass red tape and get things done. If his ideas about how to live free of prescription drugs throughout your life become popular, the pharmaceutical industry may also lose sleep (and profits) as a result. The good news is that overall; more people will be living healthy lives that are less stressful and more productive in satisfying ways. Helvie lives what he preaches; at the age of 78, he is one of the 11% of Americans above age 65 who live medication free.
Helvie grew up in the small country hamlet of Natural Dam in upstate New York, not far from the St. Lawrence River. He graduated high school in 1950 and got a job in the stock room of the hospital in the nearby town of Gouverneur (named after one of the less well-known signers of the Declaration of Independence). Curious and gregarious, he became friendly with the nurses and the hospital dietician and was informally trained to help prepare patients for surgery.
The experience was so positive, he enrolled in nursing school and began a life of service, eventually earning a doctorate in public health and wellness and becoming an educator, author, and activist for the public health sector. Helvie holds the title of Professor Emeritus of Nursing at Old Dominion University in Norfolk, Virginia, and received the Distinguished Career in Public Health Award from the American Public Health Association in 1999.
A dream sparked a significant turning point in Helvie’s life in 1974. In the dream, he received the message that he needed to get an X-ray. He had no symptoms but the X-rays revealed a spot on his lungs that was diagnosed as lung cancer. Reviewing his experience as a nurse, he surprised the doctor by refusing the prescription for surgery. The doctor responded by pronouncing, “You’ll be dead in six months.”
A friend of a friend at the National Cancer Institute had success with a program that included 2000mg laetrile, a raw fruit and vegetable diet, and an exercise program. Helvie began the regimen and incorporated his own program of prayer, meditation, and positive visualization. When asked about the controversy surrounding the use of laetrile, Helvie described how the body uses certain enzymes involved in protein digestion to work with the laetrile.
In his experience, part of his program’s success was due to following nutrition guidelines. Eating meat or fish prevented those enzymes from being available for the laetrile. In due course, Helvie was pronounced cancer-free and has been cancer-free ever since.
The importance of living a holistic life; “lifestyle is very important in staying healthy; incorporate spirituality and enjoy what you’re doing in life. If you’re not staying positive, you’re not attracting positivity back to you.”
In the 1990s, Helvie was asked to sit on the board of an agency serving homeless women. After two years of reviewing and making policy, he decided he wanted to be more active and began visiting the homeless shelter checking blood pressure and discussing health issues with the residents. He brought his students to help with the volume of people needing attention and eventually obtained a grant to open a clinic and provide more consistent service.
Until that time, most homeless people were not able to afford early treatment for their health issues and would wind up in the emergency wards when their condition became life-threatening and required more time and more resources to treat.
Developing an effective clinic became a community project. To extend the life of the grant, Helvie was able to get doctors to donate their services; the local hospital provided free lab services and pharmacies filled prescriptions for cost plus $4. Chronic diseases such as diabetes were caught earlier and supplies were available to keep the homeless healthier.
Ironically future funding was denied because of a national need for more nurses; the funds went towards education and scholarships and the clinic had to close. Helvie later assessed that the cost of running the clinic was much less than the financial burdens endured by emergency rooms and other services that had to be employed when people waited until they were very sick to seek help. You can read more in Helvie’s book, Homelessness in the United States, Europe 1999.
In his book, Healthy Holistic Aging, Helvie outlines the importance of living a holistic life; “lifestyle is very important in staying healthy; incorporate spirituality and enjoy what you’re doing in life. If you’re not staying positive, you’re not attracting positivity back to you.” Helvie wants you to live a healthy and medication-free life. When he was interviewed for this article, he stated, “I was saved from lung cancer years ago for a reason; I am a resource for people.”
As a lung cancer survivor[4][5] he has focused on holistic alternative integrative health and wellness interventions. A major part of his career also focused on education, practice and research with homeless and low-income individuals and families. He has published books, articles, and research findings in these three areas.
Helvie, C, (1975) Self-Assessment of Current Knowledge in Community Health Nursing. New York: Medical Examiners Publishing Co.
Helvie, C. (1981) Community Health Nursing: Theory and Process New York: Harper & Row Co.
Helvie, C. (1991) Community Health Nursing: Theory and Practice, New York: Springer Publishing Co.
Helvie, C. (1998) Advanced Practice Nursing in the Community, Thousand Oaks, California: Sage Publishing Co
Helvie, C and Kunstmann, W. (1999) Homelessness in the United States, Europe, and Russia, Connecticut: Greenwood. June
Clark, C (editor in chief), Gordon, R. (contributing editor), Harris, B. and Helvie, C. (advisory contributing editors) (1999) Encyclopedia of Alternative Health Practices. New York, Springer Publishing Co
Helvie, C. (2000) “The homeless, health promotion and nursing centers.” Community Health Promotion (C.C.Clarke, editor) New York:Springer
Helvie, C. (2002) “Home care for the seriously ill in the United States.” In Ambuant vor stationär. Perspektiven für eine integrierte ambulante Pflege Schwerstkranker (Schaeffer, D. and Ewers, M., Editors). Bern: Huber Verlag. Germany
Helvie, C. (2002) “Community Mobilization and Participation.” In Health Promotion in Communities (C.C. Clark, Editor). New York, Springer. Pg 69–82.
Helvie, C. (2002) “Health Promotion in a Homeless Center.” In Health Promotion in Communities. (C.C. Clark, Editor). New York: Springer. Pg 461–464.
Helvie, C. (2007) Healthy Holistic Aging: A Blueprint for Success, Minnesota: Syren Publications.
Helvie, C (2012) You Can Beat Lung Cancer: Using Alternative/Integrative Interventions. with chapters by Dr Bernie Siegel, Dr Francisco Contreras, Dr James Forsythe, Dr Kim Datzell, and Tanya Harter Pierce, London: Ayni Books.
^ Helvie, C. and Cayce, C.T. (1997) Alternative treatment for lung cancer and irregular heart beat-Two case Studies. Alternative Health Practitioner. Vol 3, No 3, Fall-Winter, 185-194.









 Do you have Lung Cancer?
Do you have Lung Cancer? Exactly How The Author Has Survived Lung Cancer For Over 22 Years And Counting
Exactly How The Author Has Survived Lung Cancer For Over 22 Years And Counting



 **Visit
**Visit 
 Let’s break free from the ordinary and strive for greatness together!
Let’s break free from the ordinary and strive for greatness together! 





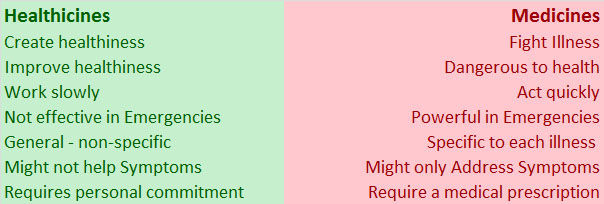




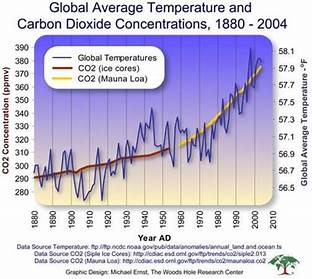






![Hospice Nurse Julie: A pacemaker is totally fine to continue to stay on during the dying process. It interacts with the electrical system in the heart. So, it will not continue to pace someone if the heart is no longer beating. So, that is not an issue; that can stay on. A defibrillator shocks a heart if it goes into dysrhythmia (an irregular heartbeat). [Dysrhythmias are] a natural process of the death and dying process, and we shouldn't worry about them. But the defibrillator should be turned off because if the person does go into an irregular rhythm during the dying phase, that person could be shocked, and being shocked is uncomfortable. So, just to be clear, it's normal for the heart to go into irregular rhythms at the end of life. Hence why it's important to have the defibrillator shut off so the person is not shocked if it goes into those irregular rhythms. Those irregular rhythms will not cause suffering, but the shocking of the defibrillator will cause suffering. So before someone comes to hospice, they should have their defibrillator turned off, which can happen in a cardiologist's office. Charday Penn / Getty Images](https://ci3.googleusercontent.com/meips/ADKq_NaZeVhn9nxmhRMjAWFvfFwjFzWIBhAmfmXqDdE1ZYfLS93X2BOkwxqqTmo4697SacEkrv_lVMCPKQpaiJ0lG4Incd-IXGZ0uFxLzJCz2kxLoMf2Z1D1GJXT9cgCYZvkuC3BF1wp7fuehOM=s0-d-e1-ft#https://img-s-msn-com.akamaized.net/tenant/amp/entityid/BB1kw4hO.img?w=768&h=512&m=6 "Hospice Nurse Julie: A pacemaker is totally fine to continue to stay on during the dying process. It interacts with the electrical system in the heart. So, it will not continue to pace someone if the heart is no longer beating. So, that is not an issue; that can stay on. A defibrillator shocks a heart if it goes into dysrhythmia (an irregular heartbeat). [Dysrhythmias are] a natural process of the death and dying process, and we shouldn't worry about them. But the defibrillator should be turned off because if the person does go into an irregular rhythm during the dying phase, that person could be shocked, and being shocked is uncomfortable. So, just to be clear, it's normal for the heart to go into irregular rhythms at the end of life. Hence why it's important to have the defibrillator shut off so the person is not shocked if it goes into those irregular rhythms. Those irregular rhythms will not cause suffering, but the shocking of the defibrillator will cause suffering. So before someone comes to hospice, they should have their defibrillator turned off, which can happen in a cardiologist's office. Charday Penn / Getty Images")

![Hospice Nurse Julie: This is a great question. Okay. So, number one, this person did the right thing. A lot of times, we feel like we have to say something to make the person feel better. Generally speaking, allowing someone to say their fears, and either just being silent and holding their hand and allowing them to have that and not try to push it away, like 'No, no, no, no, no, don't be afraid. Don't be afraid,' it's better. From my experience, allow that [fear] to happen, hold their hand, and be there with them, and maybe even answer truthfully. Whatever the truth is for them, right? 'I'm afraid too. I can see how you're afraid. And I'm so sorry. I feel afraid to.' Or what I usually say, if this is helpful, I normalize how normal it is for people to feel afraid. A lot of times just verbalizing that fear can loosen the grips that fear has on you... I think there's something about connecting together in mutual fear, right? It's okay to fear things. It doesn't necessarily mean it's wrong. It just means that it's it's unknown, and it's scary. And that, 'I'm so sorry you're feeling like that. I'm here with you. I understand. I heard it's really normal to have that fear.' Hispanolistic / Getty Images](https://ci3.googleusercontent.com/meips/ADKq_NbHopESIL-tk1XMkzIOseTpgrL6sDUaYqZaB0FzKUrVYlV6RJjgKcU8a-WeIWAL1eze73DElaKJJ18sdTw3ZoopcrXd4v6QdmnAJ6reSsdSOI0kJeKHFh-iR9DTGtib_EdWdmTEuxq-hnQ=s0-d-e1-ft#https://img-s-msn-com.akamaized.net/tenant/amp/entityid/BB1kwbuy.img?w=768&h=504&m=6 "Hospice Nurse Julie: This is a great question. Okay. So, number one, this person did the right thing. A lot of times, we feel like we have to say something to make the person feel better. Generally speaking, allowing someone to say their fears, and either just being silent and holding their hand and allowing them to have that and not try to push it away, like 'No, no, no, no, no, don't be afraid. Don't be afraid,' it's better. From my experience, allow that [fear] to happen, hold their hand, and be there with them, and maybe even answer truthfully. Whatever the truth is for them, right? 'I'm afraid too. I can see how you're afraid. And I'm so sorry. I feel afraid to.' Or what I usually say, if this is helpful, I normalize how normal it is for people to feel afraid. A lot of times just verbalizing that fear can loosen the grips that fear has on you... I think there's something about connecting together in mutual fear, right? It's okay to fear things. It doesn't necessarily mean it's wrong. It just means that it's it's unknown, and it's scary. And that, 'I'm so sorry you're feeling like that. I'm here with you. I understand. I heard it's really normal to have that fear.' Hispanolistic / Getty Images")



 Helvie grew up in the small country hamlet of Natural Dam in upstate New York, not far from the St. Lawrence River. He graduated high school in 1950 and got a job in the stock room of the hospital in the nearby town of Gouverneur (named after one of the less well-known signers of the Declaration of Independence). Curious and gregarious, he became friendly with the nurses and the hospital dietician and was informally trained to help prepare patients for surgery.
Helvie grew up in the small country hamlet of Natural Dam in upstate New York, not far from the St. Lawrence River. He graduated high school in 1950 and got a job in the stock room of the hospital in the nearby town of Gouverneur (named after one of the less well-known signers of the Declaration of Independence). Curious and gregarious, he became friendly with the nurses and the hospital dietician and was informally trained to help prepare patients for surgery.