
Alzheimer’s disease in the United States (2025 prediction) | CNN
 There is no specific timeline linked to “asking for their mom”
There is no specific timeline linked to “asking for their mom”
When a person with dementia starts calling out for their mother, it does not reliably predict how long they have left.
People can show this behavior:
- Months or even years before the end
- During moments of fear or confusion
- When they’re seeking comfort or familiarity
- When their memory has shifted back to childhood
It’s an emotional signal, not a medical indicator.
It sounds like you’re going through something painful, and I want to approach this gently.
When someone with dementia begins asking for their mom—especially if their mother has long since passed—it’s often a sign of deep confusion, fear, or a need for comfort. It does not reliably indicate how much longer they will live.
Here’s what we can say in general terms:
What “asking for their mom” can mean
- A return to early memories as recent ones fade
- Seeking safety or reassurance
- Feeling scared, lonely, or disoriented
- Progression of cognitive decline
These behaviors can appear months or even years before the end of life, or sometimes only in moments of distress. It varies widely from person to person.
 End‑of‑life signs in dementia (general, not predictive)
End‑of‑life signs in dementia (general, not predictive)
People in the final stage of dementia often show:
- Very limited speech
- Sleeping most of the day
- Difficulty swallowing
- Major weight loss
- Inability to walk or sit up
- Increased infections
Even with these signs, timelines are unpredictable. Some people decline quickly; others remain stable for long periods.
 If you’re caring for someone
If you’re caring for someone
What matters most is comfort, safety, and connection. If someone is asking for their mom, responding with warmth—“You’re safe, I’m here with you”—can help soothe them.
If you’re worried about how close they may be to the end, a doctor, nurse, or hospice team can give you clearer guidance based on what they’re seeing.
You don’t have to carry this alone. If you want to tell me more about what’s happening with your loved one, I’m here to talk through it with you.
What does tend to signal late‑stage or end‑of‑life dementia
While every person is different, the following changes are more closely associated with the final stage:
- Very little speech or only a few words
- Sleeping most of the day
- Trouble swallowing or refusing food
- Significant weight loss
- Inability to walk or sit up
- Repeated infections
- Cool hands/feet, changes in breathing
Even with these signs, the timeline can still range from weeks to many months.
Why “asking for mom” happens
It often reflects:
- A need for safety
- Emotional distress
- Loss of recent memories
- Reverting to early life memories
Responding with reassurance—“You’re safe, I’m here”—can help soothe them.
 If you’re caring for someone right now
If you’re caring for someone right now
You’re carrying something heavy. If you’re noticing other changes besides calling for their mom, a doctor, nurse, or hospice team can give you a clearer sense of where they are in the progression.
If you want to tell me a bit about what your loved one is doing or how they’ve been changing, I can help you make sense of what you’re seeing.
I can walk you through this gently. Late‑stage dementia brings very real changes, and understanding them can help you prepare emotionally and practically.
Here’s a clear, compassionate overview.
 Common Symptoms of Late‑Stage Dementia
Common Symptoms of Late‑Stage Dementia
People in the final stage of dementia typically need full‑time care. The body and brain are slowing down, and several systems begin to decline.
Sundowners syndrome, also known as sundowning, is a pattern of increased confusion, agitation, and restlessness in people with dementia, typically occurring in the late afternoon and evening.
Overview
Sundowners syndrome is not a disease itself but a set of behaviors and symptoms often seen in individuals with Alzheimer’s disease or other forms of dementia. It usually manifests as the sun sets, though symptoms can occur at other times as well. Approximately 20–45% of people with Alzheimer’s experience some form of sundowning during the course of their illness.
Sundowner’s syndrome: Symptoms, causes, treatment tips, and more
Behavioral changes: pacing, wandering, rocking, shadowing (following a caregiver closely), yelling, crying, or aggression
Emotional changes: anxiety, fear, irritability, sadness, restlessness
Cognitive changes: confusion, disorientation, paranoia, hallucinations, delusions
Sleep disturbances: difficulty falling asleep or staying asleep, insomnia
These symptoms often worsen in the late afternoon and evening, potentially leading to increased caregiver stress and a higher risk of accidents or injury.
Causes and Triggers
The exact cause of sundowning is not fully understood, but several factors may contribute:
Disrupted circadian rhythms or internal body clock changes
Fatigue from mental or physical activity during the day
Low lighting and shadows, which can increase confusion and hallucinations
Environmental changes or unfamiliar surroundings
Stress or frustration observed in caregivers
Sleep disorders or insufficient rest
Sundowning is more common in the middle stages of dementia and may subside as the disease progresses. alz.org
Management Strategies
While sundowning cannot always be prevented, several strategies can help manage symptoms:
Maintain a consistent daily routine for waking, meals, and bedtime Web.MD
Schedule activities such as appointments, bathing, or exercise in the morning or early afternoon when the person is more alert
Optimize lighting in the home during late afternoon and evening to reduce shadows and confusion
Encourage rest and relaxation during the day to reduce fatigue
Minimize stress by remaining calm and avoiding confrontations
Medication may be considered only under a doctor’s guidance if behavioral symptoms are severe
Caregivers are encouraged to observe patterns in behavior to identify triggers and adjust the environment or routine accordingly.
Key Takeaway
Sundowners’ syndrome is a common and challenging aspect of dementia care, characterized by late-day confusion, agitation, and emotional distress. Understanding triggers, maintaining routines, and creating a supportive environment can help reduce its impact on both the individual and their caregivers.
Cleveland Clinic
 Cognitive and Communication Changes
Cognitive and Communication Changes
- Very limited speech — sometimes only a few words or none at all
- Difficulty recognizing loved ones
- Loss of awareness of time, place, or surroundings
- Increased confusion, even in familiar environments
 Physical Decline
Physical Decline
- Inability to walk; eventually unable to sit up without support
- Muscle stiffness or rigid limbs
- Trouble holding up their head
- Increased risk of falls (earlier in the stage)
 Eating and Swallowing Problems
Eating and Swallowing Problems
- Difficulty chewing or swallowing (dysphagia)
- Coughing or choking while eating
- Reduced appetite
- Significant weight loss
- Dehydration
These changes often lead to discussions about comfort‑focused care.
 Changes in Sleep and Alertness
Changes in Sleep and Alertness
- Sleeping most of the day
- Very limited periods of wakefulness
- Low responsiveness
 Breathing and Body Changes
Breathing and Body Changes
- Irregular breathing patterns
- Periods of rapid breaths followed by pauses
- Cool hands and feet
- Skin mottling (patchy discoloration) near the end
 Infections and Medical Complications
Infections and Medical Complications
- Frequent infections, especially pneumonia or urinary tract infections
- Difficulty recovering from even minor illnesses
 Emotional and Behavioral Changes
Emotional and Behavioral Changes
- Anxiety or agitation
- Calling out for familiar people (like a parent)
- Restlessness
- Moments of calm or clarity mixed with confusion
A gentle reminder
These symptoms don’t appear all at once, and they don’t give a precise timeline. Some people remain in late‑stage dementia for months or even years, while others decline more quickly.
If you’re seeing some of these signs in someone you love, it’s completely understandable to feel overwhelmed.
You’re doing something incredibly hard.
If you want, you can tell me what changes you’ve noticed, and I can help you understand what they might mean. Alzheimer’s does not always begin with mild cognitive impairment (MCI). And most MCI never becomes Alzheimer’s — it can be caused by vascular issues, depression, medication or sleep disorders. Some people with MCI stay stable; a small percentage even improve
. And most MCI never becomes Alzheimer's — it can be caused by vascular issues, depression, medication or sleep disorders. Some people with MCI stay stable; a small percentage even improve (stock)")
New ‘triple threat’ cause of dementia discovered… scientists say it occurs decades before symptoms
Story by Cassidy Morrison Health Features Editor
New research points to the effects someone’s risky behavior in their 20s has on their cognitive health in their 50s and beyond.
University of Michigan researchers followed people from age 18 through their 50s and 60s, tracking people with ‘triple threat’ habits – smoking daily, binge drinking or using cannabis frequently.
A daily smoking habit in young adulthood predicted worse self-reported memory by age 50, regardless of whether the person had quit by age 35.
For binge drinking and cannabis, the harm to memory was indirect: heavy use in young adulthood raised the odds of developing a substance use disorder by midlife, and that disorder directly damaged cognitive health.
Dr Megan Patrick, principal investigator of the Monitoring the Future Panel Study, said: ‘Substance use has both acute and long-term effects on health and well-being. Poor memory is a common sign of early dementia.
‘Identifying the risk factors that can lead to dementia is crucial for the prevention and treatment of cognitive decline.’
Previous studies have linked midlife memory complaints to later dementia risk. The Michigan researchers did not diagnose cognitive decline.
Rather, they asked participants how they felt about their memory, then looked back at substance use decades earlier.
The study, published in the Journal of Aging and Health, used data from the Monitoring the Future (MTF) Longitudinal Panel Study.
While the study did not administer objective cognitive tests, such as memory or executive function exams, it used poor self-rated memory as a validated early indicator of cognitive decline.
Researchers asked 16,000 Americans from age 18 into their 50s and 60s a single question: ‘Would you say your memory is excellent, very good, good, fair, or poor?’ Anyone who answered ‘fair’ or ‘poor’ was considered to have poor self-rated memory.
Participants were surveyed repeatedly between the ages of 18 and 30, with each survey period covering roughly two years. At each wave, people reported how often they drank, smoked or used cannabis.
Researchers then counted how many of those waves a person engaged in heavy use, such as daily smoking, binge drinking or using cannabis 20 or more times a month.
Throughout the study, researchers tracked how many of those substance use waves occurred in participants’ lives.
By midlife, about one in 10 reported that their memory was ‘fair’ or ‘poor.’
In young adulthood, participants averaged two waves of binge drinking, defined as having five or more drinks in a row in the past two weeks.
They averaged just over one wave of daily smoking and less than one wave of heavy alcohol use — drinking 20 or more days a month — or frequent cannabis use, which involves using 20 or more days a month.
Alcohol use disorder, meanwhile, is defined as meeting two or more diagnostic criteria for problem drinking over the past five years, including loss of control, cravings or continued use despite harm to oneself.
By age 35, more than a quarter of participants showed signs of alcohol use disorder, six percent had cannabis use disorder — meaning their use of marijuana had caused significant life problems or loss of control — and nine percent smoked a pack of cigarettes or more a day.
The numbers might look small at first glance, but what makes them significant is that these risks did not fade after a few years. They lasted decades.
A person who engaged in heavy alcohol use in their 20s was not just at slightly higher risk of memory problems in their 30s. Each wave of heavy drinking raised the odds by 13 percent, and that risk persisted 30 to 40 years later, when they reached their 50s and 60s.
The study found that for binge drinking in young adulthood, the link to poor memory disappeared once researchers accounted for whether someone had developed alcohol use disorder by age 35.
That suggests that people who binge drank in their 20s but stopped before midlife, and never developed a disorder, likely faced no lasting impact on their memory decades later.
However, for those whose heavy drinking, whether frequent or episodic, continued into their 30s and led to alcohol use disorder by age 35, the effect was significant.
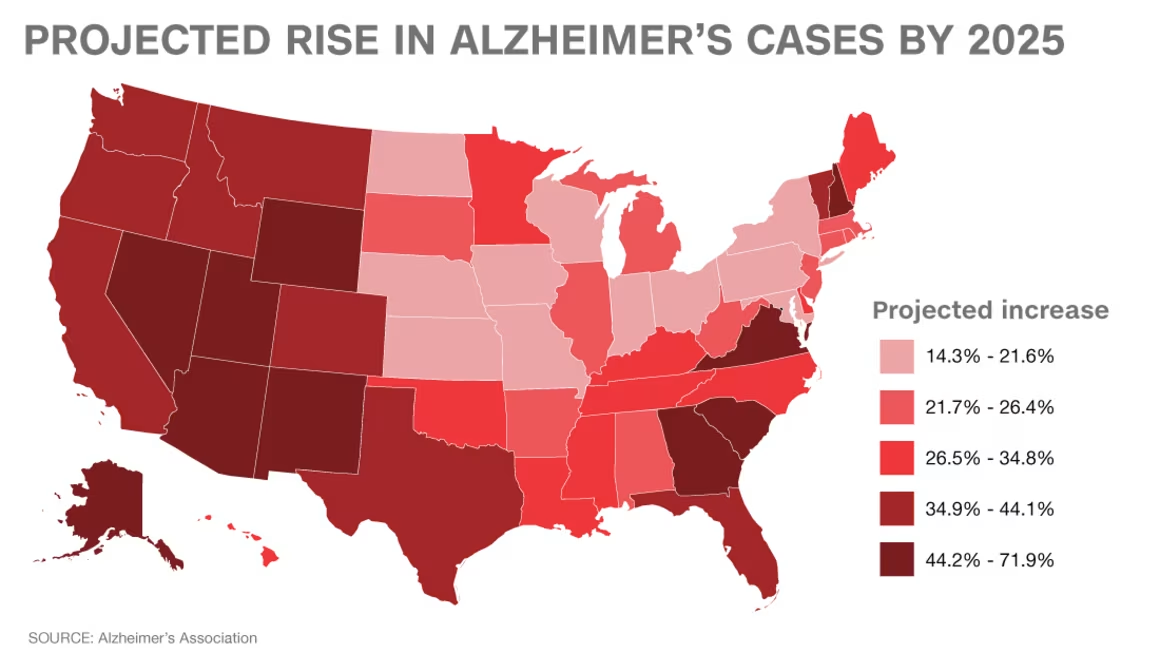
 who have dementia. The disease is most prevalent in the Southeastern US")
The map, unrelated to the latest study from the University of Michigan, shows the percentages of Medicare enrollees (people 65 and up) who have dementia.
Dementia is more common in the Southeast largely because the region has higher rates of the conditions and demographics that increase dementia risk. Research consistently shows that age, chronic health problems, and social factors all cluster more heavily in this part of the U.S., which helps explain the pattern.
Below is a clear breakdown of what the evidence shows.
Which US States Have the Highest Risk of Dementia? – Newsweek
County-Level-Prevalence-AAIC-2023
Why Dementia Is More Prevalent in the Southeast U.S.
1. Higher proportions of older adults
Age is the strongest known risk factor for dementia. Counties in the Southeast often have larger populations of adults 65+, including more people over 85, which increases overall prevalence.
2. Demographic patterns linked to higher risk
Studies show that:
- Black Americans have about 2× the risk of Alzheimer’s compared to White Americans.
- Hispanic Americans have about 1.5× the risk. These groups make up a larger share of the population in many Southeastern counties.
This demographic distribution alone raises the expected prevalence.
3. Higher rates of chronic health conditions
The Southeast has long been known as part of the “Stroke Belt” and “Diabetes Belt.” Conditions strongly associated with dementia—such as:
- Stroke
- High blood pressure
- Diabetes
- Obesity
are more common in this region. These illnesses increase the risk of vascular dementia and Alzheimer’s disease.
4. Lower average educational attainment
Lower levels of education are linked to higher dementia risk, likely because education builds “cognitive reserve” that protects the brain. Many high‑prevalence counties in the Southeast have lower average education levels, which contributes to higher dementia rates.
5. Lifestyle and environmental factors
Research suggests that regional lifestyle patterns—such as higher smoking rates, poorer access to preventive healthcare, and environmental stressors—may also contribute. Even after adjusting for health and demographic factors, geography itself remained a strong predictor of dementia risk in large studies.
 Summary Table
Summary Table
| Factor | How It Raises Dementia Rates | Evidence |
|---|---|---|
| Older population | More people in high‑risk age groups | |
| Higher % of Black & Hispanic residents | Groups with higher average risk | |
| More chronic diseases | Stroke, diabetes, hypertension increase dementia risk | |
| Lower education levels | Lower cognitive reserve | |
| Lifestyle/environment | Smoking, limited healthcare access |
If you’d like, I can also break down specific states, county‑level data, or explain how these factors might affect someone you know.
People with alcohol use disorder at 35 were 32 percent more likely to report poor memory in late midlife compared to those who drank without disorder.
People who used cannabis frequently in young adulthood were more likely to report poor memory decades later — an eight percent increase in risk for each wave of heavy use. This was the first phase of the analysis.
But when researchers accounted for midlife cannabis use disorder, that link vanished, meaning young adult use itself wasn’t the direct cause. Rather, young adult users were more likely to develop the disorder, and that disorder caused the memory problems.
Heavy marijuana use in one’s 20s raised the odds of developing cannabis use disorder by age 35.
And those who developed the disorder were 36 percent more likely to report poor memory later in life compared to those who used cannabis without developing a disorder.
In other words, frequent cannabis use in young adulthood only mattered if it continued into midlife and became a disorder. If it did not, there was no lasting impact on memory.
Cigarettes were different.
People who smoked daily during more waves of young adulthood were significantly more likely to still be smoking later in life. For each additional wave of daily smoking in their 20s, they were nearly twice as likely to be smoking a pack or more a day at 35.
But cigarettes diverged from alcohol and cannabis. Even after accounting for midlife smoking, each additional wave of daily smoking in young adulthood raised the odds of poor memory decades later by about five percent.
In other words, the damage from cigarettes appears to come from cumulative exposure in young adulthood itself, not from whether the habit continued into midlife. Quitting by age 35 did not erase the risk.
The human brain continues developing well into a person’s mid-20s, particularly in regions responsible for impulse control, decision-making and long-term planning —the functions needed for someone to recognize when a habit is becoming a problem.
During this window of heightened neuroplasticity, the brain is highly sensitive to rewards and more easily rewired by substances like alcohol, cannabis, and nicotine.
Occasional experimentation, over repeated exposure, strengthens neural pathways that reinforce compulsive use, making it harder to stop even as consequences mount.
Roughly 28 million Americans have alcohol use disorder, nearly 19 million have cannabis use disorder and approximately 29 million smoke cigarettes, making each condition a major public health threat.
An estimated seven million Americans, meanwhile, live with Alzheimer’s Disease.
That figure is slated to double by 2060, driven by the rapid aging of the baby boomer population as well as an overall rise in the number of Americans living into old age — the leading risk factor of the disease.
Read more New ‘triple threat’ cause of dementia discovered… as scientists say it occurs decades before symptoms | Daily Mail Online
This type of exercise is linked to better brain health, study finds
Unregulated blood pressure is a cause of dementia – Search
Can head trauma cause Parkinson’s disease – Search
Can head trauma cause Alzheimer’s disease – Search
Can head trauma cause depression – Search
Can head trauma cause dementia – Search
Can head trauma cause epilepsy – Search