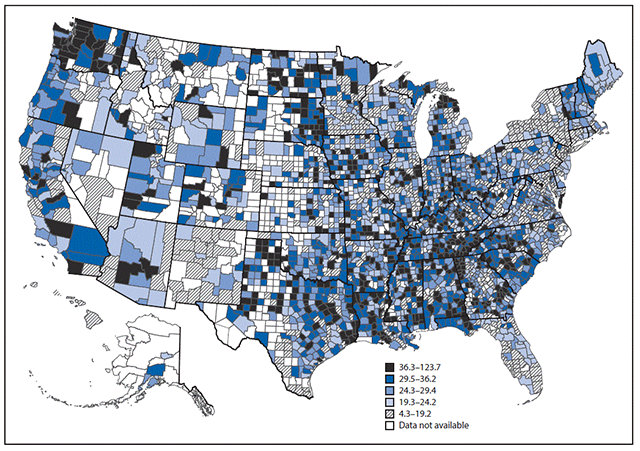
Map Shows States With the Highest Alzheimer’s Disease Deaths
Story by Marni Rose McFall
Alzheimer’s disease is a devastating neurodegenerative disorder affecting millions of Americans, and its impact varies significantly across the country.
While the disease is a nationwide concern, certain areas, particularly in the South and the Pacific Northwest, experience significantly higher mortality rates, according to data from 2022 released by the Centers for Disease Control and Prevention. Factors such as healthcare access, lifestyle, and underlying health conditions may contribute to these variations.
The CDC researchers also looked at where people with Alzheimer’s were living when they died of the disease. They found that although most deaths in 2014 occurred in nursing homes or other long-term care facilities, more patients with the disease were dying at home than they were 16 years earlier.
In 1999, only 13.9 percent of people with Alzheimer’s were living at home when they died. That number rose to 24.9 percent in 2014. Another 6.1 percent died in a hospice facility.
Possible reasons for increase
“The number of Alzheimer’s deaths has increased, in part, because of a growing population of older adults,” write the CDC researchers. They also point out that the rise in deaths from Alzheimer’s disease may be the result of fewer “competing” deaths from heart disease and stroke.
In addition, Alzheimer’s is now much more likely to be correctly diagnosed — and cited on death certificates as the direct cause of death — than in past decades.
Whatever the reasons for the increase in the nation’s Alzheimer’s death rate, the growing burden of the disease on American families is clear.
“In 2015, caregivers of persons with dementia, including Alzheimer’s, provided 18.2 billion hours of unpaid assistance,” write the researchers. “These caregiving hours might correspond to increased financial costs for caregivers and decreased work productivity, as caregivers might take leave from work to ensure adequate care is provided.”
“As Alzheimer’s disease progresses, caregiving becomes very important,” explained Christopher Taylor, a CDC epidemiologist who led the study, in the released statement. “Caregivers and patients can benefit from programs that include education about Alzheimer’s disease, how to take care of themselves and their loved one, and case management to lessen the burden of care.”
“Supportive interventions can lessen the burden for caregivers and improve the quality of care for people with Alzheimer’s disease,” he added.
What Is Alzheimer’s Disease?
The National Institute on Aging defines Alzheimer‘s disease as a progressive brain disorder that gradually destroys memory, thinking skills, and the ability to perform simple tasks.
It is most common in people over 65, with late-onset Alzheimer’s being the predominant form. In rare cases, early-onset Alzheimer’s can occur between a person’s 30s and mid-60s. The disease is the leading cause of dementia among older adults.
Named after Dr. Alois Alzheimer, who first observed abnormal clumps (amyloid plaques) and tangled fibers (tau tangles) in the brain of a woman with memory loss and erratic behavior, these features remain key indicators of the disease today.
Alzheimer’s is marked by the buildup of plaques and tangles, as well as the loss of connections between neurons that transmit messages within the brain and to other parts of the body. The damage initially impacts areas critical to memory, such as the entorhinal cortex and hippocampus, before spreading to regions responsible for language, reasoning, and social behavior.
Over time, this widespread brain deterioration severely impairs cognitive and physical abilities, leading to the loss of independence in those affected. While scientists continue to investigate other complex brain changes that may contribute to Alzheimer’s, plaques, tangles, and neuronal damage remain central to understanding the disease. Alzheimer’s Risk Higher If Mom Had Memory Problems
The top five states with the highest Alzheimer’s mortality rates are:
Mississippi
Washington
Alabama
Arkansas
Louisiana
Idaho
Utah
Georgia
Texas
California
What Causes the State Differences?
According to research from the University of Alabama, Alzheimer’s disease disproportionately affects the Deep South, where states like Alabama, Georgia, Louisiana, Mississippi, and South Carolina see significantly higher rates of dementia.
People born in this region have a 20–30 percent greater risk of developing Alzheimer’s or other forms of dementia, largely due to underlying health disparities. Factors such as high rates of hypertension, diabetes, obesity, and vascular disease in the region contribute to cognitive decline and increase dementia risk. These conditions are particularly prevalent among African Americans, who make up over 20 percent of the population in the Deep South, and face twice the risk of late-onset Alzheimer’s compared to other groups.
A key issue in addressing Alzheimer’s disparities is the underrepresentation of African Americans in Alzheimer’s-related research. Although African Americans make up around 10 percent of the U.S. population over 55, few clinical studies have included a proportionate number of African American participants.
The Deep South is also a hotspot for other health conditions that heighten the risk of Alzheimer’s, including cerebrovascular disease, diabetes, and obesity. The so-called “Stroke Belt” – Searchand“Diabetes Belt” – Search—areas in the region where those diseases are prevalent—contribute to widespread vascular problems and cognitive decline, while obesity is linked to inflammation that could exacerbate dementia.
A spokesperson for UsAgainstAlzheimer’s said, “There are a number of comorbidities that can increase a person’s risk of developing Alzheimer’s or related dementias and controlling these can reduce a person’s risk of developing Alzheimer’s. We should be clear that hypertension and diabetes are not really “lifestyle factors” but diseases that can be treated—and they should be treated.”
“One of the things we are focused on is making sure the public knows there are things people can do to reduce their risk of Alzheimer’s. Hypertension, diabetes, social isolation, and tobacco use, to name a few, are examples of the risk factors. But people can make simple lifestyle changes to reduce their risk. Exercise, sleep, eating a healthy diet, and even wearing hearing aids if you have hearing loss are just some of the actions people can take to reduce the risk of developing Alzheimer’s.”
“Access to information and healthcare are two of the biggest challenges,” the spokesperson said.
“Working with the Centers for Disease Control, we are working very hard to reach these very communities so we can raise Alzheimer’s awareness and encourage people to talk about it. But you still have the issue of access to healthcare and adequate treatment – not only for dementia but to address the other factors that increase the risk for Black and Latino people, in particular. We need a healthcare system that works for everyone; getting there is a major priority for ‘UsAgainstAlzheimer’s.” – Search
Update, 17/10/24, 12:01 p.m. ET: This article was updated with comment from UsAgainstAlzheimer’s.
Estimate of U.S. prevalence of adults aged 18 and over with any serious medical condition, as of 2018. (CDC map)
A new report from the Centers for Disease Control and Prevention has a map showing which counties have populations with an increased risk of severe outcomes from covid-19. Many are rural, since rural populations tend to be older, more obese, and are more likely to have underlying medical conditions.
I have a special interest in Alzheimer’s disease. For nearly 25 years, I practiced general neurology in Portland, Oregon, and some of my patients had dementia. In 2012, while doing a genealogical DNA search, I inadvertently discovered that I have two copies of the APOE-4 allele, meaning I had a very good chance of getting Alzheimer’s-caused dementia by age 80.
I felt Gobsmacked.
I remember walking down the stairs in a daze after reading the report from the genetic testing service and telling my wife, Lois, “I think I am screwed.”
A year later, I retired at age 62 even though I had no symptoms of cognitive impairment. If I had almost any other job, I could have continued working for a few more years, but in medicine, forgetfulness could have fatal consequences. I suddenly wore two hats — that of a retired physician who had cared for a lot of people with Alzheimer’s disease and now a person living with the same disorder.
I had been taught, in medical school in the 1970s and even during my neurology residency in the 1980s, that Alzheimer’s disease progresses from onset to death in about three to five years, and nothing can be done about it. Neither statement is true.
In hindsight, my first symptom of Alzheimer’s disease was a gradual loss of smell that I first noticed in 2006. This was accompanied by odd olfactory hallucinations that smelled like baking bread mixed with perfume. I didn’t have any measurable cognitive impairment until 2015, when I had significant trouble remembering words, including the names of friends and colleagues.
I had a PET scan as part of a research study, which showed my brain had the beginning of abnormal tau protein, a key part of diagnosing Alzheimer’s. When the scans were repeated in 2018 and 2022, the tau protein can be seen spreading through my brain.
We now know that the first signs of Alzheimer’s disease, beta-amyloid plaques, can be seen in the brain up to 20 years before any cognitive changes. Tau-containing tangles start to form later, about two or three years before the onset of mild cognitive impairment. There is a variation in the speed of progression from mild impairment to full-blown dementia to death, probably about eight to 12 years on average.
I am now 73, and I have had mild cognitive impairment for roughly five years, followed by mild dementia for about four years. We don’t yet have a way to stop this progression, but what have I been doing to slow it?
There are lifestyle modifications that help, and they also decrease the likelihood of getting it in the first place.
Top among them is aerobic exercise.
Multiple studies have shown up to a 50 percent reduction in the chance of getting Alzheimer’s disease for people who exercise regularly. The only group that doesn’t seem to benefit from exercise are those who already have dementia. The sooner you start, the better.
I started exercising daily in 2012 as soon as I learned that I was on the Alzheimer’s trajectory. Recent evidence shows that tai chi can help people who already are experiencing cognitive impairment.
The data for adopting a plant-based diet are almost as strong as exercise. I follow a variant of the Mediterranean diet called the MIND diet that includes eating foods with increased flavonols such as nuts and certain vegetables. Many experts now recommend avoiding alcohol, especially for people with a family history of dementia. Recently, I gave up my daily glass of beer or wine. Frankly, I have been surprised that nonalcoholic beer tastes quite good.
Staying mentally active is very important. For me, my most important brain exercise is reading and writing. I do a crossword puzzle every day while eating lunch, and I enhance the brain benefit by looking up words I don’t know. Staying socially engaged is important but increasingly difficult as dementia progresses. It’s best for me to socialize with just one or two people at a time. Getting at least 7½ hours of sleep each night appears to reduce the chance of getting dementia.
What about drugs?
We now have two FDA-approved drugs, lecanemab and donanemab, that are effective in removing beta-amyloid from the brain, but they only slow cognitive decline by about 35 percent. They can also have lethal side effects in patients with two copies of the APOE-4 allele, like me. After only four monthly injections of aducanumab (a cousin of lecanemab) during the phase 3 trial, I developed swelling and bleeding in my brain requiring a stay in an intensive care unit and about four months to recover. The drug has since been discontinued by its manufacturer.
These treatments represent an important step forward in understanding the neurobiology of Alzheimer’s disease, but they should not be used by everyone. So I have learned that Alzheimer’s disease is not the rapidly progressive dementia I was taught about in medical school. It is a slowly progressive disease that is asymptomatic for up to 20 years. Mild symptoms of cognitive impairment may be annoying but usually can allow normal activities for another five years or so.
Even work may be possible with accommodations. Once someone has dementia, unable to live independently, lifestyle modifications and medications do not seem to be as effective. In my experience, it is critical to manage Alzheimer’s disease in the early stages to postpone the onset of dementia. Don’t wait for the horses to get out of the barn.
How to lower your dementia risk as cases expected to rise by 2060
Research shows that dementia cases are going up, with a study released this week estimating that cases in the United States, for instance, will double by 2060.
The study, published in the journal Nature Medicine on Monday, found that the risk of developing dementia after age 55 is double that reported by previous studies, estimating it at 42 per cent. They said this was tied to population ageing.
Previous research has estimated that global cases of dementia will rise due to population ageing and growth including a 2022 study that estimated global cases could rise from 57.4 million cases in 2019 to nearly 153 million in 2050.
Western Europe would see an estimated 74 per cent increase in cases by 2050, central Europe would have an 82 percent increase, and eastern Europe would see a 92 per cent increase, according to the study.
But people can take steps to reduce their risk of dementia, such as controlling high blood pressure and other bad-for-the-brain health problems, and it’s not too late to try even in middle age.
“All of our research suggests what you do in midlife really matters,” said Dr Josef Coresh, the study’s co-author from New York University (NYU) Langone Health in the US.
Dementia isn’t only Alzheimer’s
Dementia is the progressive loss of memory, language, and other cognitive functions.
Alzheimer’s is the most common form, and silent brain changes that eventually lead to it can begin two decades before symptoms appear. Other types include vascular dementia when heart disease or small strokes impair blood flow to the brain.
Many people have mixed causes, meaning vascular problems could exacerbate brewing Alzheimer’s symptoms.
Measuring the risk from a certain age over the potential remaining life span can guide public health recommendations and medical research.
“It’s not a guarantee that someone will develop dementia,” said Dr James Galvin, a University of Miami Alzheimer’s specialist. He wasn’t involved with the new study but said the findings fit with other research.
Dementia risk is different by age
Prior studies estimated about 14 percent of men and 23 percent of women would develop some form of dementia during their lifetime.
Coresh’s team analysed more recent data from a US study that has tracked the heart health and cognitive function of about 15,000 older adults for several decades. Importantly, they found the risk changes with the decades.
Only 4 percent of people developed dementia between the ages of 55 and 75, what Coresh calls a key 20-year window for protecting brain health.
For people who survive common health threats until 75, the dementia risk then jumps to 20 per cent by age 85 and 42 per cent between ages 85 and 95.
Overall, the lifetime dementia risk after age 55 was 35 per cent for men and 48 per cent for women, the researchers concluded.
Women generally live longer than men, a main reason for that difference, Coresh noted. Black Americans had a slightly higher risk, 44 per cent, than white people at 41 per cent.
Ways to lower dementia risk
There are some risk factors people can’t control, including age and whether you inherited a gene variant called APOE4 that raises the chances of late-in-life Alzheimer’s.
But people can try to avert or at least delay health problems that contribute to later dementia.
Coresh, for example, wears a helmet when biking because repeated or severe brain injuries from crashes or falls increase the risk of later-in-life dementia.
Especially important: “What’s good for your heart is good for your brain,” added Miami’s Galvin. He urges people to exercise, avoid obesity, and control blood pressure, diabetes and cholesterol.
For example, high blood pressure can impair blood flow to the brain, a risk not just for vascular dementia but also linked to some hallmarks of Alzheimer’s.
Similarly, the high blood sugar of poorly controlled diabetes is linked to cognitive decline and damaging inflammation in the brain.
Stay socially and cognitively active, too, Galvin said. He urges people to try hearing aids if age brings hearing loss, which can spur social isolation.
“There are things that we have control over, and those things I think would be really, really important to build a better brain as we age,” he said.
“To the world, you might be one person, but to one person, you might be the world”
Genetic risk for Alzheimer’s disease and dementia appeared to be partly offset by high levels of cardiorespiratory fitness, U.K. Biobank data suggested.
Overall, high cardiorespiratory fitness was associated with better global and domain-specific cognitive functions and lower risk of dementia in both middle-age and older adults, reported Weili Xu, PhD, of the Karolinska Institute in Stockholm, and co-authors.
The incidence rate ratio (IRR) of all-cause dementia was 0.60 (95% CI 0.48-0.76) for high versus low cardiorespiratory fitness.
Dementia onset was delayed by 1.48 years (95% CI 0.58- 2.39) in the high fitness group.
Among people with moderate or high genetic dementia risk scores, high cardiorespiratory fitness attenuated dementia risk by 35% (IRR 0.65, 95% CI 0.52-0.83) compared with low fitness, Xu and colleagues said in the British Journal of Sports Medicine.
“Cardiorespiratory fitness may be used as a predictor of cognitive health,” the researchers stated. “Enhancing cardiorespiratory fitness could be a strategy for the prevention of dementia, even among people with a high genetic predisposition for Alzheimer’s disease.”
No study to date has explored the combined effect of cardiorespiratory fitness and genetic risk on dementia, Xu and colleagues pointed out. “Open questions remain regarding whether and to what extent favorable cardiorespiratory fitness may reduce dementia risk, even in those with a high genetic predisposition for dementia,” they noted.
In this analysis, the researchers followed 61,214 dementia-free U.K. Biobank participants ages 39-70 for a median of 11.72 years.
Mean baseline age was 56 and 52% of participants were female.
A 6-minute submaximal exercise test on a stationary bike was completed at study enrollment (from 2006 through 2010) to estimate cardiorespiratory fitness. Fitness scores were divided into low, moderate, and high tertiles, standardized by age and sex.
Global and domain-specific cognitive function was evaluated at baseline. Dementia was identified over the follow-up period using medical history and medical records. Genetic predisposition for dementia was estimated using polygenic risk scores for Alzheimer’s disease derived from genome-wide association studies.
During the follow-up period which spanned to 12 years, 553 people (0.9%) received a diagnosis of dementia. High cardiorespiratory fitness was associated with a lower risk of dementia and a delay in the onset of dementia across middle and older ages.
In multi-adjusted linear regression models, higher cardiorespiratory fitness was associated with better global cognitive function, prospective memory, verbal/numeric memory, and processing speed in all participants. The association between cardiorespiratory fitness and cognitive function was consistent in different age and genetic risk groups.
“Future research on the relationship between cardiorespiratory fitness and brain health, especially in older adults, is warranted, and the mechanisms by which cardiorespiratory fitness modifies the relationship between genetic risk and dementia deserve further investigation,” Xu and colleagues observed.
“As the measurement of cardiorespiratory fitness in clinical settings becomes both important and feasible, cardiorespiratory fitness may be used as a routine health monitoring tool or an indicator of health conditions,” they added.
The study was observational and cannot determine causality. Also, U.K. Biobank participants often are healthier than the general population, the researchers acknowledged.
U.K. Biobank participants with certain health conditions — such as chest pain at rest, high weight, high blood pressure, or a pacemaker — were excluded from the exercise test, which may have influenced outcomes. The submaximal exercise test used in this study is considered less accurate than maximal exercise testing which requires participants to exercise to exhaustion, Xu and co-authors said.
In addition, incident dementia cases were determined through register information, which might have led to an underestimation. Most participants did not have repeated cardiorespiratory fitness measurements, and relationships between changes in cardiorespiratory fitness and dementia risk could not be determined.
This research was supported by the Swedish Research Council, the Swedish Council for Health Working Life and Welfare, and the Karolinska Institutet Research Foundation.
Xu and co-authors reported no conflicts of interest.
People who have a genetic predisposition to Alzheimer’s disease may lower their risk of developing the illness with a workout routine, according to a new report. The study found that men and women with high levels of cardiorespiratory fitness in middle age and beyond were 35 percent less likely to develop Alzheimer’s disease or other forms of dementia in old age compared to their less fit peers. The benefits of exercise were particularly pronounced in those at increased genetic risk of Alzheimer’s because they carried the APOE-E4 gene variant or other genetic factors that predispose to the disease.
“Enhancing cardiorespiratory fitness could be a strategy for the prevention of dementia, even among people with a high genetic predisposition for Alzheimer’s disease,” the authors stated. The findings were published in the British Journal of Sports Medicine.
For the study, researchers from the Karolinska Institute in Stockholm and other medical centers analyzed health records from 61,214 men and women who were part of the UK Biobank, a database containing in-depth genetic and medical information from half a million British citizens over many years. They ranged in age from 39 to 70 at the start of the study period, from 2006 to 2010.
At the beginning of the study period, participants underwent a six-minute fitness test on a stationary bicycle to assess their cardiorespiratory fitness, a measure of the ability of the heart, blood and lungs to supply oxygen to muscles during physical exertion. They were grouped into low, medium or high levels of cardiorespiratory fitness, standardized according to their age and sex.
Researchers assessed individuals’ genetic risk for Alzheimer’s disease, according to standard research-based DNA analyses of genes linked to the disease. Participants also underwent tests of memory and thinking skills to assess their cognitive health. All were free of Alzheimer’s disease or other forms of dementia when the study began.
Participants were followed for about 12 years, including with follow-up cognitive tests. During that time, 553 of them developed Alzheimer’s disease or another form of dementia.
The researchers found that overall, the more aerobically fit someone was in middle age, the better their cognitive health was more than a decade later. Cardiorespiratory fitness seemed to benefit multiple facets of memory, such as recalling specific words, names and numbers or remembering specific tasks, such as making an appointment.
The greatest benefits were observed in individuals with a genetic predisposition for Alzheimer’s. Those with the highest levels of cardiorespiratory fitness had a 35 percent lower relative risk of developing the disease compared to their least fit peers. Aerobic fitness delayed the onset of dementia by the equivalent of about one-and-a-half years, the researchers found.
“Our study shows that higher cardiorespiratory fitness is associated with better cognitive function and decreased dementia risk,” the authors concluded. “Moreover, high cardiorespiratory fitness may buffer the impact of genetic risk of all dementia by 35 percent”
The study was observational and cannot prove cause and effect. But it involved a large study population, and earlier research has shown that greater cardiorespiratory fitness is linked to a lower risk of serious diseases such as heart disease, stroke or cancer and a lower risk of dying young.
Cardiorespiratory fitness declines by around 3 percent to 6 percent per decade when we are in our 20s and 30s, but the decline accelerates to more than 20 percent per decade by the time we reach our70s.
Experts say the best way to help minimize cardiorespiratory decline as we age is by choosing an activity you enjoy, such as walking, running, biking or a dance or spin class, and to do it regularly for at least half an hour several days a week. Aim to perform the activity at a fairly rigorous level, in which it would be difficult to hold a conversation with a friend. You can also mix it up, aiming for brief periods of high-intensity exercise amid longer periods of lower intensity exertion.
If you’re just getting started, see your doctor to make sure the exercise plan is right for you. And don’t forget other lifestyle factors that can promote brain health, including a heart-healthy diet and a good night’s sleep.
By ALZinfo.org, The Alzheimer’s Information Site. Reviewed by Eric Schmidt, Ph.D. Fisher Center for Alzheimer’s Research Foundation at The Rockefeller University.
Source: Shuqi Wang, Liuao Xu, Wenzhe Yang, et al: “Association of cardiorespiratory fitness with dementia risk across different levels of genetic predisposition: a large community-based longitudinal study” British Journal of Sports Medicine, November 19, 2024
As the mind’s delicate gears interlock and whirl, anxiety and stress lurk like saboteurs, potentially hastening the onset of dementia’s fog. This poignant imagery encapsulates the complex interplay between mental health and cognitive decline, a relationship that has garnered increasing attention from researchers and healthcare professionals alike. The connection between anxiety, stress, and dementia is not merely coincidental but represents an intricate web of neurological and physiological processes that can significantly impact an individual’s cognitive health over time.
Anxiety and dementia, while distinct conditions, often intertwine in ways that can profoundly affect a person’s quality of life. Anxiety, characterized by persistent worry and fear, is a common mental health disorder that affects millions worldwide. Dementia, on the other hand, is a broad term encompassing various neurodegenerative disorders that lead to cognitive decline, with Alzheimer’s disease being the most prevalent form. The prevalence of anxiety in dementia patients is strikingly high, with studies suggesting that up to 71% of individuals with dementia experience significant anxiety symptoms.
Understanding the relationship between anxiety, stress, and dementia is crucial for several reasons. First, it can help in early identification of individuals at higher risk of developing dementia. Second, it opens up new avenues for potential interventions that could slow down or even prevent cognitive decline. Lastly, it underscores the importance of mental health in overall brain health, challenging the traditional view that cognitive decline is an inevitable part of aging.
The Link Between Anxiety and Dementia
The connection between anxiety and dementia is multifaceted, involving various physiological and psychological mechanisms. Understanding anxiety and its effects on cognitive function is crucial to grasping this relationship. Anxiety can impact cognitive performance in several ways, including:
1. Impaired attention and concentration 2. Reduced working memory capacity 3. Slower processing speed 4. Difficulties in decision-making
These cognitive effects, when persistent over time, may contribute to an increased risk of developing dementia. Several studies have shown a correlation between anxiety and dementia risk. For instance, a meta-analysis published in the journal Alzheimer’s Research & Therapy found that individuals with anxiety had a 57% higher risk of developing dementia compared to those without anxiety.
The potential mechanisms connecting anxiety and dementia are still being investigated, but several theories have emerged:
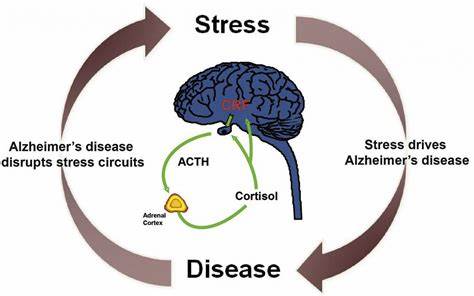
1. Chronic stress response: Anxiety triggers a prolonged stress response, leading to elevated cortisol levels that can damage brain cells over time.
2. Inflammation: Anxiety is associated with increased inflammation in the body, including the brain, which is a known risk factor for dementia.
3. Vascular changes: Anxiety can affect cardiovascular health, potentially leading to reduced blood flow to the brain and increasing the risk of vascular dementia.
4. Sleep disruption: Anxiety often interferes with sleep quality, and poor sleep has been linked to an increased risk of cognitive decline.
5. Neuroplasticity: Chronic anxiety may impair the brain’s ability to form new neural connections, a process crucial for maintaining cognitive health.
Can Stress Make Dementia Worse?
To understand how stress impacts dementia, it’s essential to first define stress and its effects on the brain. Stress is the body’s response to any demand or challenge, triggering a cascade of physiological changes. While acute stress can be beneficial in certain situations, chronic stress can have detrimental effects on brain health.
Research has shown that stress can indeed exacerbate dementia symptoms. The hidden link between stress and memory loss becomes more apparent in individuals with dementia. Stress can worsen cognitive symptoms such as memory loss, confusion, and difficulty with problem-solving. Moreover, it can amplify behavioral symptoms like agitation, anxiety, and depression in dementia patients.
The physiological changes in the brain due to chronic stress are significant and can contribute to the progression of dementia:
1. Hippocampal atrophy: Chronic stress can lead to shrinkage of the hippocampus, a brain region crucial for memory formation and already vulnerable in dementia.
2. Amyloid-beta accumulation: Stress has been shown to increase the production of amyloid-beta, a protein associated with Alzheimer’s disease.
3. Tau protein aggregation: Stress can accelerate the formation of tau tangles, another hallmark of Alzheimer’s disease.
4. Oxidative stress: Chronic stress increases oxidative stress in the brain, leading to cellular damage and potentially accelerating cognitive decline.
5. Neuroinflammation: Stress triggers inflammatory responses in the brain, which can exacerbate neurodegenerative processes.
The Impact of Stress on Dementia Progression
The effects of stress on cognitive decline in dementia patients are profound and multifaceted. The complex relationship between stress and Alzheimer’s disease reveals that stress can accelerate the rate of cognitive decline in individuals already diagnosed with dementia. This acceleration is thought to occur through various mechanisms:
1. Exacerbation of existing pathology: Stress can worsen the underlying neurodegenerative processes in dementia.
2. Cognitive reserve depletion: Stress may deplete cognitive reserve, reducing the brain’s ability to compensate for damage.
3. Behavioral changes: Stress-induced behavioral changes can interfere with daily functioning and quality of life.
Stress-induced inflammation plays a significant role in dementia progression. Chronic stress activates the body’s inflammatory response, leading to the release of pro-inflammatory cytokines. These inflammatory molecules can cross the blood-brain barrier and contribute to neuroinflammation, a key factor in the progression of neurodegenerative diseases.
Several case studies have demonstrated the effects of stress on dementia. For example, a study published in the journal Neurology followed a group of dementia patients over two years and found that those experiencing high levels of stress showed a more rapid cognitive decline compared to those with lower stress levels. Another study in the American Journal of Geriatric Psychiatry reported that dementia patients exposed to acute stressors, such as hospitalization or the death of a spouse, experienced significant worsening of cognitive symptoms in the following months.
Managing Anxiety and Stress in Dementia Patients
Given the significant impact of anxiety and stress on dementia, managing these factors is crucial in dementia care. Non-pharmacological interventions for anxiety reduction in dementia patients have shown promising results and include:
1. Cognitive Behavioral Therapy (CBT): Adapted for individuals with cognitive impairment, CBT can help manage anxiety symptoms.
2. Mindfulness and relaxation techniques: These practices can help reduce stress and improve overall well-being.
3. Music therapy: Listening to familiar music can reduce anxiety and improve mood in dementia patients.
4. Art therapy: Engaging in creative activities can provide a sense of accomplishment and reduce stress.
5. Pet therapy: Interaction with animals has been shown to reduce anxiety and improve mood in dementia patients.
Lifestyle changes to minimize stress are equally important for both dementia patients and their caregivers:
1. Establishing routines: Predictable daily schedules can reduce anxiety and confusion.
2. Regular physical exercise: Exercise has been shown to reduce stress and improve cognitive function.
3. Maintaining social connections: Social engagement can provide emotional support and cognitive stimulation.
4. Engaging in enjoyable activities: Participating in hobbies and pleasant activities can reduce stress and improve quality of life.
5. Ensuring adequate sleep: Good sleep hygiene is crucial for managing stress and supporting cognitive health.
The importance of support systems for patients and caregivers cannot be overstated. Understanding the link between stress and dementia is crucial for caregivers to provide effective support. Support groups, respite care, and educational resources can help both patients and caregivers manage stress and anxiety more effectively.
Prevention Strategies: Reducing Anxiety and Stress to Lower Dementia Risk
While managing anxiety and stress in dementia patients is crucial, prevention strategies aimed at reducing these factors in the general population may help lower the risk of developing dementia. Early intervention for anxiety disorders is key. Treating anxiety early in life may potentially reduce the risk of cognitive decline later on. This can involve:
1. Psychotherapy: Cognitive Behavioral Therapy (CBT) and other forms of talk therapy can effectively manage anxiety.
2. Medication: When necessary, anti-anxiety medications can be used under medical supervision.
3. Lifestyle modifications: Incorporating stress-reduction techniques into daily life from an early age.
Stress management techniques for long-term brain health are essential for everyone, regardless of their current cognitive status. These techniques include:
1. Mindfulness meditation: Regular practice can reduce stress and improve cognitive function.
2. Physical exercise: Regular aerobic exercise has been shown to reduce stress and support brain health.
3. Healthy diet: A balanced diet rich in antioxidants and omega-3 fatty acids can support brain health and reduce inflammation.
4. Adequate sleep: Prioritizing good sleep hygiene is crucial for stress management and cognitive health.
5. Time management: Effective time management can reduce daily stress and improve overall well-being.
The role of cognitive stimulation in preventing dementia should not be underestimated. Engaging in mentally stimulating activities throughout life can build cognitive reserve, potentially delaying the onset of dementia symptoms. Such activities include:
1. Learning new skills or languages 2. Engaging in challenging puzzles or games 3. Reading and writing 4. Participating in social activities and discussions 5. Pursuing creative hobbies
Conclusion
The relationship between anxiety, stress, and dementia is complex and multifaceted. Understanding stress-induced anxiety and its potential long-term consequences on cognitive health is crucial for both prevention and management of dementia. Anxiety and chronic stress can significantly impact cognitive function, potentially increasing the risk of developing dementia and accelerating its progression in those already diagnosed.
Addressing anxiety and stress in dementia care is of paramount importance. By implementing strategies to manage these factors, we may be able to improve the quality of life for dementia patients and potentially slow the rate of cognitive decline. Moreover, focusing on anxiety and stress reduction in the general population could serve as a preventive measure against dementia.
Future research directions in this field are promising and may lead to better treatments and preventive strategies. Areas of interest include:
1. Developing more targeted interventions for anxiety in dementia patients 2. Investigating the long-term effects of early anxiety treatment on dementia risk 3. Exploring the potential of stress-reduction techniques in slowing cognitive decline 4. Studying the genetic and epigenetic links between anxiety, stress, and dementia
As our understanding of the intricate relationship between mental health and cognitive decline continues to grow, there is hope for better treatments and prevention strategies. By addressing anxiety and stress throughout the lifespan, we may be able to support better brain health and reduce the global burden of dementia.
Learning how to deal with anxiety and manage stress effectively is not just about improving current quality of life, but also about investing in long-term cognitive health. As research progresses, the importance of mental health in maintaining cognitive function becomes increasingly clear, offering new avenues for intervention and prevention in the fight against dementia.
1. Gimson, A., Schlosser, M., Huntley, J. D., & Marchant, N. L. (2018). Support for midlife anxiety diagnosis as an independent risk factor for dementia: a systematic review. BMJ Open, 8(4), e019399.
2. Gulpers, B., Ramakers, I., Hamel, R., Köhler, S., Oude Voshaar, R., & Verhey, F. (2016). Anxiety as a Predictor for Cognitive Decline and Dementia: A Systematic Review and Meta-Analysis. The American Journal of Geriatric Psychiatry, 24(10), 823-842.
3. Justice, N. J. (2018). The relationship between stress and Alzheimer’s disease. Neurobiology of Stress, 8, 127-133.
4. Machado, A., Herrera, A. J., de Pablos, R. M., Espinosa-Oliva, A. M., Sarmiento, M., Ayala, A., … & Cano, J. (2014). Chronic stress as a risk factor for Alzheimer’s disease. Reviews in the Neurosciences, 25(6), 785-804.
5. Mah, L., Binns, M. A., & Steffens, D. C. (2015). Anxiety symptoms in amnestic mild cognitive impairment are associated with medial temporal atrophy and predict conversion to Alzheimer’s disease. The American Journal of Geriatric Psychiatry, 23(5), 466-476.
6. Orgeta, V., Qazi, A., Spector, A. E., & Orrell, M. (2014). Psychological treatments for depression and anxiety in dementia and mild cognitive impairment. Cochrane Database of Systematic Reviews, (1).
7. Sindi, S., Kåreholt, I., Johansson, L., Skoog, J., Sjöberg, L., Wang, H. X., … & Kivipelto, M. (2018). Sleep disturbances and dementia risk: A multicenter study. Alzheimer’s & Dementia, 14(10), 1235-1242.
8. Terracciano, A., Sutin, A. R., An, Y., O’Brien, R. J., Ferrucci, L., Zonderman, A. B., & Resnick, S. M. (2014). Personality and risk of Alzheimer’s disease: New data and meta-analysis. Alzheimer’s & Dementia, 10(2), 179-186.
9. Wilson, R. S., Begeny, C. T., Boyle, P. A., Schneider, J. A., & Bennett, D. A. (2011). Vulnerability to stress, anxiety, and development of dementia in old age. The American Journal of Geriatric Psychiatry, 19(4), 327-334.
10. Yaffe, K., Vittinghoff, E., Lindquist, K., Barnes, D., Covinsky, K. E., Neylan, T., … & Marmar, C. (2010). Posttraumatic stress disorder and risk of dementia among US veterans. Archives of General Psychiatry, 67(6), 608-613.
Caring for someone with Alzheimer’s is one of the toughest jobs in the world. “It is stressful, physically and emotionally draining, and very expensive, as almost 15 million unpaid caregivers for people with Alzheimer’s and other dementias can attest,” says Dr. Scott McGinnis, medical editor of the Harvard Special Health Report A Guide to Coping with Alzheimer’s Disease.
How to take care of a person with dementia
Learning how to take care of a person with dementia can be a trial-and-error process. Every person with dementia and every caregiver is unique, and so is their relationship. However, the following general tips may be useful in helping people with dementia remain physically healthy and connected to the world.
Help people with dementia by speaking simply and patiently. To get the person’s attention, begin by using his or her name. Use simple phrasing and short sentences, but be careful to avoid talking to the person as if he or she were a child. Give someone with Alzheimer’s time to complete a sentence or thought, and try not to interrupt.
Make mealtimes less stressful. Reduce sensory confusion at meals. See that the dining area is well lit. Make sure the person is comfortably seated and doesn’t need to use the bathroom. Keep items that may be mistaken for food, like dog biscuits or flower bulbs, out of sight.
Serve nourishing, manageable meals. Use a plate color that contrasts with the food. Remove condiments from the table. Limit choices by putting only one food on the plate at a time and offering only one utensil. (Curved spoons, divided plates, and straws can make it easier for people to feed themselves.) Don’t serve food or drink that is too hot. Cut food into small pieces. Remind the person to eat slowly and chew each bite thoroughly. If he or she chokes easily, switch to soft foods. Serve foods containing fiber to help prevent constipation.
Reduce resistance to bathing. Avoid discussing whether a bath is needed. Prepare everything in advance. Lay out towels, soap, shampoo, and clothes. Have the water ready and at the right temperature before bringing him or her into the bathroom. Be calm, gentle, and reassuring. If the person seems disturbed at this invasion of privacy, cover portions of his or her body with a towel. Encourage him or her to do as much as possible without hands-on help. Talk through each step. If the person refuses to get into the tub or shower, be flexible and suggest an alternative. If all else fails, try again later.
Accident-proof the bathroom. Use rubber tub mats, tub seats, grab bars, nonslip bath mats, etc. Do not use bath oil or products that make the tub slippery. Put razors and electrical appliances out of reach. Take the lock off the bathroom door.
Incorporate skin care into bath time. Check the skin for rashes and sores. Use powder or cornstarch to prevent chafing, and apply body lotion to dry skin.
Simplify dental care. Prepare the toothbrush and demonstrate how to brush. If the person will not brush and refuses assistance, give him or her a cloth moistened with mouthwash and tell the person to rub it over his or her teeth.
Dementia is a disease that affects millions of people across the globe every year. It is often a highly misunderstood condition that is marred by numerous misconceptions, which make the condition difficult to understand and study.
You should know that dementia is not a name for an illness, rather it is a collective term that describes a broad range of symptoms that relate to declining thinking, memory, and cognitive skills. These symptoms have deteriorating effects that usually affect how a patient acts and engages in the day-to-day activities.
In advanced dementia stages, affected persons may experience symptoms that bring out a decline in rational thought, intellect, social skills, memory, and normal emotional reactivity. It is something that can make them powerless when it comes to living normal, healthy lives.
Relatives, caregivers, spouses, siblings, children and anyone close to a person who has dementia need to know how to deal with behavioral problems that surface because of the illness. Examples of dementia problems may include aggressiveness, violence and oppositional behaviors. Find out some of the vital Do and Don’ts when dealing with a dementia patient.
Dealing with Dementia Behavior: Do’s
We have identified a list of 9 Do’s that you should keep in mind when dealing with behavior problems associated with dementia. They are as follows:
Do Try and Identify the Trigger that Causes Behavior Change
After spending some time with a patient who has dementia, caregivers may be in a position to identify some of the things that make dementia sufferers yell, get physical, or change their mood. For some, it may be something simple such as taking a bath or even getting dressed.
The best approach to handle this is not to force the patient to do something that they do not want to do. Try and distract them with something else that allows them to relax and calm down. Once they are not a danger to themselves or anyone around them, try going back to the subject, but this time reassuringly and calmly.
Do Keep Eye Contact When Speaking
Communicating with a dementia patient requires a lot of patience, especially during later stages of dementia. It is vital to ensure that you talk in a place that has good lighting, a place that is quiet and without too many distractions. Do not try to stand over the person you are talking to, but rather try to be at their level and keep eye contact at all times. Take care to make sure that body language is relaxed and open. Prepare to spend quality time with the person so that they do not feel rushed or like they are a bother.
Do Introduce Yourself
It does not matter how many times you have to do it. Dementia comes with memory loss which means that the patient may forget your name. When starting a conversation, always remind them your name and tell them something nice that will make them smile.
Do Stick to Routine
Scientists state that habits belong to their own memory structure, which remains intact for long periods even when the patient loses their most recent memory skills. Routine helps dementia patients to know what to do on a daily basis. Caregivers should strive to include meaningful activities in the routine for as long as possible as a way of ensuring that the person with the condition has a sense of independence and purpose in life.
Remember to continually re-examine the routine to remove things that may agitate, depress or make the dementia patient feel unsettled. Sadly, it may reach a point where people with dementia may not be able to keep up with a basic routine. However, as long as they still can, be sure that they do things every day that make them happy.
Do Offer Assurance Often
Many times, people with dementia may experience feelings of isolation, fear, loneliness or confusion. They may not be able to express this in the right way and thus may wander off or keep saying that they want to go back home, especially if they are in a senior living facility. This is not the time to shut them out. It’s a good idea to assure them that they are safe and in a good place.
If you are close enough, provide a comforting hug every once in a while and remind them that they are in a place that has their best interest at heart. Where possible, engage in exercise or take a walk as even light physical activity may help to reduce agitation, restlessness and anxiety.
Do Make Sure That the Dementia Patient Gets Enough Rest, Food and Water
Fatigue, hunger and thirst may cause combativeness. Ensure that the person with dementia is well fed, hydrates enough, and gets adequate sleep and rest. In line with this, they should also have enough bathroom breaks. Research also shows that it may help to reduce loud noises as well as clutter in the space where the patient spends most of his/her time, as both loud noises and clutter tend to over-stimulate people with dementia.
Do Share Photos
At times, the behavior that dementia patients exhibit is because they are missing a person or place they love. Experts suggest for caregivers to go through as many photos as possible with the person with the illness. It is a tool that helps to stimulate happy memories while the dementia sufferer goes down the memory lane.
Going through family photos has been known to play a significant role when it comes to the patients remembering the pleasant times they had. Family photos also help people with dementia to remember special people in their lives. It is best to use large pictures that have clear labels because many people who have dementia often have declining or poor eyesight. Try and select meaningful moments, and you can also make it an activity where patients can create scrapbooks with the people they love.
Do Try to be Pleasant
Caregivers are also humans who are prone to emotions like anger, stress, impatience, and irritation. Even when one goes through caregiver burnout, it is best that the patient does not get wind of it. It is better to step out of the room and try some breathing exercises to calm down before going back to deal with the dementia patient. Where possible, shelve the “bad” feelings and try to deal with them later. Dementia patients deal with a lot and they do not need more on their plate if they are to lead fulfilling and happy lives.
Do try to be Forgiving and Patient
Do not forget that dementia is the condition that results in irrational behavior and causes dementia sufferers to act the way they do. The patients demand plenty of patience and forgiveness from the people looking after them. Have the heart to let things go instead of carrying grudges around for something that the patient may not be in control of.
Dealing with Dementia Behavior: Don’ts
There are certain actions you should not take and certain things you should not do when you are dealing with dementia behavior problems. We have identified a list of 10 such Don’ts, and they are:
Do Not Engage in Arguments
One of the worst things a person can do to an individual who has dementia is to start an argument or even force them to do something that makes them upset or angry. When the discussion or argument is too heated, it may be better to walk away to create an environment where everyone can remain calm. Experts agree that one of the ways that can yield results when it comes to dementia behavior problems is to get rid of the word no when dealing with patients. Avoid forcibly restraining a dementia sufferer at all costs.
Do Not Be Impolite
Communication and language often become difficult over time for individuals who have dementia. It is therefore very important to use polite language when speaking with someone who has dementia. Do not use sharp or threatening voices. Do not feel frustrated when you have to repeat words or phrases several times because the person you are conversing with does not catch them or understand as fast as they should. Restrain from ridiculing or patronizing the patients about what they say.
Do Not Keep Correcting the Patient
People with dementia do not like it when someone keeps correcting them every time they say something that may not be right. It makes them feel bad about themselves and can make them drift out of the conversation. Discussions should be humorous and light and one should always speak slowly and clearly using simple and short sentences to capture and keep the interest of the dementia patients.
Do Not Get Angry or Upset
When looking after persons with dementia, practicing self-control is of utter importance. Learn how to breathe in and just relax without taking things personally or getting angry and upset. Remember that dementia patients do not act the way they do out of their own accord. It is the illness that makes them behave the way they do.
Do Not Try and Alter Undesirable Behavior
Lack of understanding may push one to try and change or stop any undesirable behavior from patients who have dementia. Keep in mind that it is almost impossible to teach new skills or even reason with the patient. Try instead to decrease frequency or intensity of the behavior. For instance, respond to emotion and not the changes in behavior. If a patient insists on always asking about a particular family member reassure them that he or she is safe and healthy as a way of keeping them calm and happy.
Do Not Try to Stop a Person Who Wants to Leave a Room
Staying in one place for long periods may result in behavior problems in the dementia patient. It is essential to have a safe environment where they can enjoy the outdoors without any problem. When someone tries to leave a room, do not force them to stop. Doing this may result in an extreme reaction such as severe distress or injuries.
Instead, it is best to accompany the patient so that they are safe. You can even suggest going for a drive around the block so that they can experience a new environment for a short period. If they do not want company, just let them go but stay close by to make sure that the patient is safe at all times.
Do Not Expect Too Much
It helps to have an open mind when dealing with an individual who has dementia. Try and keep up with their pace without having to rush them too much. It is advisable to avoid trying to teach new information or ask the affected individuals to do something that they have not previously done.
Do Not Shy Away From Asking For Help
No one may have all the answers especially when it comes to taking care of a person with dementia. Try doing research on how their behavior changes and what needs to be done to help them live their lives without too many complications. Hire help when it becomes too much as it also ensures that you do not become too frustrated or drained.
When you have multiple family members who can help, ask everyone to pitch in and look after the patient so that you can get some personal space to breathe and re-energize when it is your time to look after the patient. When you feel like you can no longer look after your loved one at your own home, it may be time to consider assisted living. In such cases, look into dementia care homes that can provide specially trained professionals.
Do Not Panic
When a dementia patient becomes aggressive or agitated, try to remain in control without breaking down, panicking and using physical force. Try other approaches that may help to make them calm. These can include holding their hand firmly but gently, singing them their favorite song, or patting their pack gently. Note that some people do not like to be touched; thus, it is best to give them some space by sitting away from them or leaving the room until they calm down.
Do Not Ignore Physical Abuse
As much as one needs to be tolerant, kind, forgiving, and patient with older adults who have dementia, it does not mean that they have to excuse the patients when they become physically aggressive and allow the abuse to continue. It is not to be accepted, and if it happens, it is best to alert your doctor who will work on the solution to make sure it stops. It will keep both the patient and caregiver in safety.
From physical manifestations to angry outbursts, taking care of an individual with dementia may not be easy. However, working with the tips above can help caregivers and loved ones to get through it. Remember that there are plenty of treatments, interventions and special care providers who can help; therefore, you should never be shy about getting help when you need it.
Infographic: Do’s and Don’ts: Communicating With a Person Who Has Alzheimer’s Disease
People with Alzheimer’s disease may have trouble finding the right words or remembering what they want to say. This can make communication difficult. Use the tips below to better communicate with a person who has Alzheimer’s.
To share the image, right-click on it and select “save image as” to save the file to your computer. We encourage you to use the hashtag #NIAHealth in your social media posts to connect with people and organizations with similar goals.
Alzheimer’s made my mom unable to recognize her grandkids. Breakthroughs too late for her can change the disease’s trajectory—if diagnosis and treatment start early
My mother, Margaret, was the heart of our family. When my twins were born prematurely, she moved in with us to help care for them. Her support allowed me to take on being a new mom of two and a busy career during a challenging time. And her selflessness stayed with me as I helped care for her later in life when she needed it most. gns of cognitive impairment. Within a few years, Alzheimer’s disease stole her joy for cooking, love of music, and ability to recognize her grandchildren.
My father, sisters, and I shared caregiver duties, watching her with vigilance, and balancing a new dynamic in our family. I found myself sleeping on my mother’s bedroom floor to prevent her from wandering in the night. We were a private family and did not discuss my mom’s illness very much outside our immediate circle. When caring for her, our world became small, our routine focused on keeping her safe. My sisters and I wondered, Will we be next?
It would be different if my mom were diagnosed today. Nearly two decades later, we know so much more about this disease. Improvements in detection, diagnosis, and medicines are offering new hope for slowing its progression.
Studies have confirmed we have the greatest opportunity to impact this disease in its earliest stages, when some people may initially show only subtle changes in memory and thinking that differ from normal aging. People in this state, often with mild cognitive impairment, may encounter minor challenges in everyday living, and may be younger and appear healthier than society has traditionally portrayed.
Innovations in diagnostics are now able to identify underlying disease pathology—clumps of amyloid plaques in the brain. And emerging blood tests hold promise to speed and simplify diagnosis with remarkable accuracy. Just years ago, for patients like my mom, a confirmed diagnosis wasn’t even possible until after death.
Changing perceptions of Alzheimer’s disease
Moving forward, it will take all of us—people with Alzheimer’s disease, providers, and families—to change how we view this disease and how we treat it.
More people need to be aware about the importance of the early detection of symptoms, often in the primary care setting, and reducing the stigma surrounding the disease so that more people are diagnosed.
Today it can take more than two years on average to diagnose Alzheimer’s after the first symptom is detected. We need health care providers to include cognitive assessments and advanced diagnostics routinely in their clinical practice when Alzheimer’s disease is suspected. And we must advocate for access and reimbursement for diagnostic tests as well as treatments.
We need greater equity across disease states, races, genders, and generations. Promoting available and affordable options across geographic and socioeconomic boundaries and allowing care close to home should be a priority. As a new generation of caregivers begin to take responsibility for their mothers, fathers, and families, we should make sure these newly diagnosed individuals are helped as early in their disease as possible.
The progress we are now realizing will lead to more investment and research in Alzheimer’s disease that will unlock further understanding and open the door to address other neurodegenerative conditions. This moment will be a catalyst to drive progress toward understanding diseases such as ALS, Parkinson’s, and multiple sclerosis.
This is all within our reach: What were breakthroughs in science and care in cancer and cardiovascular disease in previous decades are now routine in how we treat these patients today. The same can be true in neurodegenerative disease.
Looking back on my mom’s experience, I remain deeply grateful that she continued to recognize my dad, my sisters, and me through the end of her life. When I held her hand and looked into her eyes as she passed away, I found comfort in knowing that she did not see a stranger, but a loving daughter who had felt a lifetime of love and care.
Scientific breakthroughs came too late for my mom. but they are not too late for people diagnosed today. The story of Alzheimer’s is now being rewritten. We have the chance to truly change the trajectory of this disease for many people, and we need to act with urgency to help them and those that love them.
I would have given so much to have more time with my mom, and I am so glad that many families now have that chance for more time.
I’ve been practicing medicine at a renowned institution for 40 years. Society isn’t ready for us to reverse the aging process across an entire population
The opinions expressed in Fortune.com commentary pieces are solely the views of their authors and do not necessarily reflect the opinions and beliefs of Fortune.
Learn its history and what Alzheimer’s research has discovered so far.
Also, consider investigating an Alzheimer’s clinical trial here.
Minor abnormalities, so-called amyloid plaques, and tau tangles that form in the brain and are found in specific locations throughout are two distinguishing hallmarks of Alzheimer’s Disease Dementia. Advanced testing, such as PET scans, MRI, DNA, and spinal fluid analysis, can shed invaluable light on the probability of Alzheimer’s.
Alois Alzheimer was a German psychiatrist who discovered the pathological condition of Dementia and diagnosed the disease that bears his name. Alois was born in Marktbreit, Germany, in 1864 and showed an early aptitude for science.
After obtaining his medical degree, he worked in hospitals in Frankfurt, where he met Auguste Deter, a 51-year-old woman suffering from progressive short-term memory loss. He was eventually able to isolate the pathological causes of severe Dementia, work so extensive that the condition became known as Alzheimer’s disease.
Today, it is believed that “Alzheimer’s disease (AD) is the most common form of Dementia among older people. Dementia is a brain disorder that seriously affects a person’s ability to carry out daily activities.
AD begins slowly. It first involves the parts of the brain that control thought, memory, and language. People with AD may have trouble remembering recent events or the names of people they know. A related problem, mild cognitive impairment (MCI), causes more memory problems than usual for people of the same age. Many, but not all, people with MCI will develop AD.
In AD, symptoms get worse over time. People may not recognize family members or have trouble speaking, reading, or writing. They may forget how to brush their teeth or comb their hair. Later, they may become anxious or aggressive or wander away from home. Eventually, they need total care, which can cause great stress for family members who must care for them.
AD usually begins after age 60. The risk goes up as you get older. Your risk is also higher if a family member has had the disease. No treatment can stop the disease. However, some drugs may help keep symptoms from worsening for a limited time.”
You may also be interested to read about the IDEA Study and how the results suggested that about a third of those diagnosed with Alzheimer’s disease in the past, now, due to recent advancements in imaging, were found not to have Alzheimer’s disease. Yes, they may have had significant cognitive impairments, but their cause was not necessarily Alzheimer’s disease, and the treatment plan was altered accordingly.
Lastly, a well-known study of nuns, lasting decades, has indicated that some individuals can live cognitively intact, showing no signs or clues to significant degenerative changes, despite having the hallmarks of a Dementia pathology seen at their autopsy.
November is Alzheimer’s Awareness Month, a time to also heighten awareness about Alzheimer’s disease and show support for the more than 6.2 million Americans living with it. There are a number of quick and easy ways you can help raise awareness, show support, and fight Alzheimer’s disease!
Why Teal?
Teal is the Alzheimer’s Awareness color of the Alzheimer’s Foundation of America (AFA). AFA uses teal because it has been shown in color psychology studies to be a calming color. This is helpful when designing and decorating spaces and events to be welcoming and comforting to those living with Alzheimer’s. So, next time you see someone dressed in teal, remember the more than 6 million people living with Alzheimer’s and the help they need.
‘A study to give us hope’: Lifestyle changes improve Alzheimer’s symptoms for some
Looking back, Tammy Maida, 67, said things started to change in her late 50s. At first, she would lose track of her belongings: her keys multiple times a day, a ring, eyeglasses, her purse.
She would drive to the grocery store in her hometown of San Jose, California, and forget where she parked the car. At home, she couldn’t remember where she had put the groceries. Her husband, Paul, would sometimes find them in the garage.
A lifelong, avid reader, Maida stopped picking up books because she couldn’t remember the last chapter she had read or the major characters.
“I honestly thought I was losing my mind, and the fear of losing my mind was frightening,” she told CNN Chief Medical Correspondent Dr. Sanjay Gupta for the CNN documentary “The Last Alzheimer’s Patient.”
Today, Maida is back to devouring short novels and helping with the family finances.
Another patient, Mike Carver, 71, was diagnosed with early-onset Alzheimer’s at age 64 while working as a business executive. Doctors told him to put his affairs in order with little hope for the future. Carver eventually learned that he was a carrier of both copies of the APOE4 gene, which carries the highest-known genetic risk for Alzheimer’s.
Now, however, Carver is back to reconciling the family finances and keeping track of investments. “It’s kind of like doing a happy dance,” he said with a laugh. “It was kind of hard saying that part of me was just gone. And so a lot of self-worth has come back.”
How did Maida and Carver gain back what dementia had stolen from them?
By participating in what researchers call the first randomized controlled clinical trial to use lifestyle interventions and show cognitive improvement in people with mild cognitive impairment or early dementia due to Alzheimer’s disease.
The study, published Friday in the journal Alzheimer’s Research and Therapy, was small, with only two dozen people receiving treatment and a similar number serving as controls over a short, five-month period. Not everyone showed improvement. Still, for some participants and their families, there were remarkable changes.
The thinking skills of a majority of people in the intervention group stayed the same, a boon since most in the control group declined. Ten people saw their cognition actually improve, while a blood test found levels of amyloid, a hallmark of Alzheimer’s disease, were retreating, said lead study author Dr. Dean Ornish, a clinical professor of medicine at the University of California, San Francisco.
“This is a study to give us hope,” said journalist and former California first lady Maria Shriver, founder of the Women’s Alzheimer’s Movement at Cleveland Clinic in Ohio, which provided early seed funding for the new research.
“This study finally gives us scientific data to support what many of us in this field have believed instinctively for years, that lifestyle interventions may determine the trajectory of people’s Alzheimer’s journeys,” Shriver said in a statement.
Because the clinical trial was only five months long, the results were “astounding,” said co-senior study author Rudy Tanzi, an Alzheimer’s researcher and professor of neurology at Harvard Medical School in Boston.
“If you picture a brain full of damage as a sink full of water, when you just turn off the tap, it takes a long time for that sink to slowly drain, right?” said Tanzi, director of the McCance Center for Brain Health at Massachusetts General Hospital in Boston.
“If you want the amyloid to go down in 20 weeks, as we found on one blood test, you’re going to need a Roto-Rooter.”
That’s exactly what the study did — provide people with a carefully constructed, multipart, intensive lifestyle intervention that targets multiple contributors to cognitive decline. And those who put in the most effort saw the best results.
“There was a statistically significant dose-response relationship between the degree of adherence to our lifestyle changes and the degree of improvement we saw on measures of cognition,” said Ornish, creator of the Ornish diet and lifestyle medicine program, founder and president of the nonprofit Preventive Medicine Research Institute and coauthor of “Undo It!: How Simple Lifestyle Changes Can Reverse Most Chronic Diseases.”
“I would describe this as a really positive, small pilot study, a starting point for additional research,” said Dr. Suzanne Schindler, an associate professor of neurology at Washington University School of Medicine in St. Louis.
“I wish we could do a program like this for everyone, not just people with mild cognitive impairment or early stage Alzheimer’s,” said Schindler, who was not involved in the study.
‘Eat well, move more, stress less and love more’
The lifestyle intervention Ornish created — “eat well, move more, stress less and love more” — has been tested before. In 1990, Ornish showed for the first time in a randomized clinical trial that coronary artery disease could often be reversed with nothing more than diet, exercise, stress reduction and social support.
“How is it that these same four lifestyle changes stop, and often reverse, the progression of such a wide spectrum of the most common and costly chronic diseases?” Ornish asked.
“It’s because they all share many of the same underlying biological mechanisms: chronic inflammation, oxidative stress, changes in the microbiome, changes in gene expression, changes in immune function and so on,” he said.
“And the lifestyle choices we make every day — what we eat, how we respond to stress, how much exercise we get, how much love and social support we have — can activate or downregulate these different mechanisms.”
Taking care of the heart and the brain
Since what’s good for the heart is good for the brain, Ornish asked, why couldn’t this intervention also work on early Alzheimer’s or other forms of dementia?
“If we found patients didn’t improve at all, that would be disappointing but an important finding — people need to know that,” Ornish said. “But if we found that we could slow, stop or even reverse the progression of Alzheimer’s disease, that would be an important finding as well.”
To find out, Ornish and professors from other leading academic centers began recruiting patients into a new study. Covid-19 hit, which stalled progress until the team realized it could offer the intervention via video conference calls.
“That was a game changer because before you had to live near a hospital or clinic that we trained in our program, and most people don’t,” Ornish said. “Now you can live anywhere, even a food desert or rural area.”
Fifty-one people were selected for the study, then randomized into two groups: One group would consume a vegan diet, do daily aerobic exercise, practice stress reduction and engage in online support groups for 20 weeks, while the control group would not.
A nutritionist held hour-long video classes on diet, while a therapist led equally lengthy group sessions three times a week in which participants shared their feelings and received support.
Each day a fitness instructor led online strength training exercises and encouraged 30-minute daily walks. Meditation, deep breathing, yoga and other ways to reduce stress took up another hour every day. The program also encouraged participants to prioritize good quality sleep.
Supplements were provided to everyone in the intervention group. They took a daily multivitamin, omega-3 fatty acids with curcumin, coenzyme Q10, vitamin C and B12, magnesium, a probiotic and Lion’s mane mushroom (Hericium erinaceus).
To be sure the vegan diet was followed, all meals and snacks for both the participant and spouse were delivered to their homes. Calories were unrestricted, but protein and total fat were about 18% of the daily caloric intake — experts say the average American eats twice the amount of protein they need and obtains 36% of daily calories from total fat.
Complex carbs found in whole grains, vegetables, fruits, tofu, nuts and seeds made up most of the diet.
Sugar, alcohol and refined carbs found in processed and ultra processed foods were taboo.
“The gut microbiome loves all the fiber from the whole grains, fruits and vegetables,” Tanzi said. “My lab has shown in animals that a happy gut can trigger metabolites to the brain, which induce microglial cells to eat more of the amyloid in the brain.”
Microglial cells are the brain’s housekeepers, responsible for tidying up synapses, taking out cellular trash and gobbling up nasties such as amyloid. They do most of their work at night during key stages of sleep.
But when neurons die due to injury, age or a disease such as Alzheimer’s, microglia become sidetracked, turning into killers to fend off whatever seems to be damaging the brain, Tanzi said. Doing so can unleash a cytokine storm, ramping up inflammation and causing further brain injury.
Lifestyle changes can help microglia get back on track, Tanzi said. Besides a high-fiber diet, aerobic exercise and plenty of good quality sleep also encourage microglial cells and other amyloid-clearing enzymes to do their jobs.
“Exercise and sleep induce clearance of amyloid in different ways than the gut microbiome,” Tanzi said. “Combining them is a powerful tool.”
In fact, microbiome tests of the study participants found two of the organisms that increase the risk of Alzheimer’s went down in the intervention group and up in the control group, Ornish said.
“At the same time, microorganisms believed to be protective against Alzheimer’s went up in the intervention group and down in the control group,” he added.
Improvement for some but not all
Five months into the program, the rest of the results were in. For some, such as Mike Carver and Tammy Maida, the program was life-changing.
In addition to an improvement in his cognition, Carver and his wife, Pat, lost weight and reduced their cholesterol numbers and resting heart rates. Mike’s PSA levels, a test for prostate cancer, looked better than ever before.
Maida is sleeping better and back to accomplishing the tasks she thought she had to give up due to Alzheimer’s: doing laundry, cooking, voraciously reading books, keeping track of household finances and small business bookkeeping.
“The cloud of the Alzheimer’s diagnosis slowly started to lift,” she told CNN’s Gupta. “Honestly, I am more me than I had been for the years prior to starting Dr. Ornish’s program.”
However, not everyone in the intervention improved. Two people dropped out — one couldn’t give up McDonald’s on the way home from his daily walks.
“It was only a 20-week intervention period with a small sample size of just 24 people,” said John Morris, distinguished professor of neurology and codirector of the Knight Alzheimer’s Disease Research Center at Washington University School of Medicine.
“Only 10 out of 24 people in the intervention group seemed to improve and that meant 14 did not,” said Morris, who was not involved in the study. “Overall, it’s interesting, but it would need to be a larger study, with a more representative sample and a longer treatment period to draw any definite conclusions.”
For people who did the intervention, a blood test called plasma Aβ42/40 showed an “extremely” significant improvement, the study found. The test measures the level of amyloid in the blood, a sign that the microglia in the brain are doing their job. Tests that measure amyloid in different ways did not show improvement, however.
“Unfortunately, not all the biomarkers were showing consistent effects,” said Washington University’s Schindler, who specializes in blood biomarkers.
There was no significant change in a test for amyloid called p-tau 181, considered to be a superior measure of Alzheimer’s risk, Schindler said. Nor was there any change in glial fibrillary acidic protein, or GFAP, another blood biomarker that seems to correlate reasonably well with Alzheimer’s disease.
“If one of these markers improves, you typically see all of them improve, so the fact they did not makes me wonder whether this effect is real,” she said. “If they were to repeat the study with a much larger population for a longer period of time, perhaps more change could be seen.”
Need for empowerment
One of the earliest patients recruited to the study was Cici Zerbe, now in her mid-80s. Six years ago, a neurologist diagnosed her with mild cognitive impairment and dementia due to Alzheimer’s. She knew what that meant.
“My grandmother, she would sit forever and just twiddle her thumbs and stare into space and wouldn’t talk too much,” Zerbe told Gupta, who tracked her progress for five years in the documentary.
“Her mother, they finally put her in a home because her father couldn’t take care of her,” said Zerbe’s husband, John. “My greatest fear was she would end up like her mother and grandmother, where I couldn’t take care of her.”
A lifelong runner, retired educator and matriarch of a large family, Zerbe joined Ornish’s study in 2019. Nearly 5 years later, Zerbe and her husband, who live in Novato, California, are still doing the program, and believe the intervention has turned her life around.
“It’s really helped. I think it’s slowed it down,” her daughter Alicia Manzoni told Gupta.
“I think she’s doing very well,” her husband added. “I was afraid by this time she would be in a home or something.”
After all, it’s the improvement in daily life, not blood or cognitive tests, that is most meaningful to a person with Alzheimer’s and their family, said Washington University’s Morris.
Dr. Sanjay Gupta speaks to CiCi and John Zerbe’s entire family. CiCi is shown wearing white. –
“What matters to the patient in the family is whether they’re able to do the things they normally do,” Morris said. “If they couldn’t read and now, they can read, that’s great. That’s an outstanding achievement.”
For Ornish, who has watched members of his family die from Alzheimer’s, the study’s results are important for one key reason — hope.
“So often when people get a diagnosis of dementia or Alzheimer’s, they are told by their doctors that there is no future, ‘It’s only going to get worse, get your affairs in order.’ That’s horrible news and is almost self-fulfilling,” Ornish said.
“I’m not about false hope, and I’m not saying that everyone will get better,” he added. “I’m here to empower people with the knowledge that if you do change, there is a reasonably good chance that you may slow the progression of the disease and often improve it.”
“It is stressful, physically and emotionally draining, and very expensive, as almost 15 million unpaid caregivers for people with Alzheimer’s and other dementias can attest,” says Dr. Scott McGinnis, medical editor of the Harvard Special Health Report:
Learning how to take care of a person with dementia can be a trial-and-error process. Every person with dementia and every caregiver is unique, and so is their relationship. However, the following general tips may be useful in helping people with dementia remain physically healthy and connected to the world.
Help people with dementia by speaking simply and patiently. To get the person’s attention, begin by using his or her name. Use simple phrasing and short sentences, but be careful to avoid talking to the person as if he or she were a child. Give someone with Alzheimer’s time to complete a sentence or thought, and try not to interrupt.
Make mealtimes less stressful. Reduce sensory confusion at meals. See that the dining area is well lit. Make sure the person is comfortably seated and doesn’t need to use the bathroom. Keep items that may be mistaken for food, like dog biscuits or flower bulbs, out of sight.
Serve nourishing, manageable meals. Use a plate color that contrasts with the food. Remove condiments from the table. Limit choices by putting only one food on the plate at a time and offering only one utensil. (Curved spoons, divided plates, and straws can make it easier for people to feed themselves.) Don’t serve food or drink that is too hot. Cut food into small pieces. Remind the person to eat slowly and chew each bite thoroughly. If he or she chokes easily, switch to soft foods. Serve foods containing fiber to help prevent constipation.
Reduce resistance to bathing. Avoid discussing whether a bath is needed. Prepare everything in advance. Lay out towels, soap, shampoo, and clothes. Have the water ready and at the right temperature before bringing him or her into the bathroom. Be calm, gentle, and reassuring. If the person seems disturbed at this invasion of privacy, cover portions of his or her body with a towel. Encourage him or her to do as much as possible without hands-on help. Talk through each step. If the person refuses to get into the tub or shower, be flexible and suggest an alternative. If all else fails, try again later.
Accident-proof the bathroom. Use rubber tub mats, tub seats, grab bars, nonslip bath mats, etc. Do not use bath oil or products that make the tub slippery. Put razors and electrical appliances out of reach. Take the lock off the bathroom door.
Incorporate skin care into bath time. Check the skin for rashes and sores. Use powder or cornstarch to prevent chafing, and apply body lotion to dry skin.
Simplify dental care. Prepare the toothbrush and demonstrate how to brush. If the person will not brush and refuses assistance, give him or her a cloth moistened with mouthwash and tell the person to rub it over his or her teeth.
Dementia is a disease that affects millions of people across the globe every year. It is often a highly misunderstood condition that is marred by numerous misconceptions, which make the condition difficult to understand and study.
You should know that dementia is not a name for an illness, rather it is a collective term that describes a broad range of symptoms that relate to declining thinking, memory, and cognitive skills. These symptoms have deteriorating effects that usually affect how a patient acts and engages in the day-to-day activities.
In advanced dementia stages, affected persons may experience symptoms that bring out a decline in rational thought, intellect, social skills, memory, and normal emotional reactivity. It is something that can make them powerless when it comes to living normal, healthy lives.
Relatives, caregivers, spouses, siblings, children and anyone close to a person who has dementia need to know how to deal with behavioral problems that surface because of the illness. Examples of dementia problems may include aggressiveness, violence and oppositional behaviors. Find out some of the vital Do and Don’ts when dealing with a dementia patient.
Dealing with Dementia Behavior: Do’s
We have identified a list of 9 Do’s that you should keep in mind when dealing with behavior problems associated with dementia. They are as follows:
Do Try and Identify the Trigger that Causes Behavior Change
After spending some time with a patient who has dementia, caregivers may be in a position to identify some of the things that make dementia sufferers yell, get physical, or change their mood. For some, it may be something simple such as taking a bath or even getting dressed.
The best approach to handle this is not to force the patient to do something that they do not want to do. Try and distract them with something else that allows them to relax and calm down. Once they are not a danger to themselves or anyone around them, try going back to the subject, but this time reassuringly and calmly.
Do Keep Eye Contact When Speaking
Communicating with a dementia patient requires a lot of patience, especially during later stages of dementia. It is vital to ensure that you talk in a place that has good lighting, a place that is quiet and without too many distractions. Do not try to stand over the person you are talking to, but rather try to be at their level and keep eye contact at all times. Take care to make sure that body language is relaxed and open. Prepare to spend quality time with the person so that they do not feel rushed or like they are a bother.
Do Introduce Yourself
It does not matter how many times you have to do it. Dementia comes with memory loss which means that the patient may forget your name. When starting a conversation, always remind them your name and tell them something nice that will make them smile.
Do Stick to Routine
Scientists state that habits belong to their own memory structure, which remains intact for long periods even when the patient loses their most recent memory skills. Routine helps dementia patients to know what to do on a daily basis. Caregivers should strive to include meaningful activities in the routine for as long as possible as a way of ensuring that the person with the condition has a sense of independence and purpose in life.
Remember to continually re-examine the routine to remove things that may agitate, depress or make the dementia patient feel unsettled. Sadly, it may reach a point where people with dementia may not be able to keep up with a basic routine. However, as long as they still can, be sure that they do things every day that make them happy.
Do Offer Assurance Often
Many times, people with dementia may experience feelings of isolation, fear, loneliness or confusion. They may not be able to express this in the right way and thus may wander off or keep saying that they want to go back home, especially if they are in a senior living facility. This is not the time to shut them out. It’s a good idea to assure them that they are safe and in a good place.
If you are close enough, provide a comforting hug every once in a while and remind them that they are in a place that has their best interest at heart. Where possible, engage in exercise or take a walk as even light physical activity may help to reduce agitation, restlessness and anxiety.
Do Make Sure That the Dementia Patient Gets Enough Rest, Food and Water
Fatigue, hunger and thirst may cause combativeness. Ensure that the person with dementia is well fed, hydrates enough, and gets adequate sleep and rest. In line with this, they should also have enough bathroom breaks. Research also shows that it may help to reduce loud noises as well as clutter in the space where the patient spends most of his/her time, as both loud noises and clutter tend to over-stimulate people with dementia.
Do Share Photos
At times, the behavior that dementia patients exhibit is because they are missing a person or place they love. Experts suggest for caregivers to go through as many photos as possible with the person with the illness. It is a tool that helps to stimulate happy memories while the dementia sufferer goes down the memory lane.
Going through family photos has been known to play a significant role when it comes to the patients remembering the pleasant times they had. Family photos also help people with dementia to remember special people in their lives. It is best to use large pictures that have clear labels because many people who have dementia often have declining or poor eyesight. Try and select meaningful moments, and you can also make it an activity where patients can create scrapbooks with the people they love.
Do Try to be Pleasant
Caregivers are also humans who are prone to emotions like anger, stress, impatience, and irritation. Even when one goes through caregiver burnout, it is best that the patient does not get wind of it. It is better to step out of the room and try some breathing exercises to calm down before going back to deal with the dementia patient. Where possible, shelve the “bad” feelings and try to deal with them later. Dementia patients deal with a lot and they do not need more on their plate if they are to lead fulfilling and happy lives.
Do try to be Forgiving and Patient
Do not forget that dementia is the condition that results in irrational behavior and causes dementia sufferers to act the way they do. The patients demand plenty of patience and forgiveness from the people looking after them. Have the heart to let things go instead of carrying grudges around for something that the patient may not be in control of.
Dealing with Dementia Behavior: Don’ts
There are certain actions you should not take and certain things you should not do when you are dealing with dementia behavior problems. We have identified a list of 10 such Don’ts, and they are:
Do Not Engage in Arguments
One of the worst things a person can do to an individual who has dementia is to start an argument or even force them to do something that makes them upset or angry. When the discussion or argument is too heated, it may be better to walk away to create an environment where everyone can remain calm. Experts agree that one of the ways that can yield results when it comes to dementia behavior problems is to get rid of the word no when dealing with patients. Avoid forcibly restraining a dementia sufferer at all costs.
Do Not Be Impolite
Communication and language often become difficult over time for individuals who have dementia. It is therefore very important to use polite language when speaking with someone who has dementia. Do not use sharp or threatening voices. Do not feel frustrated when you have to repeat words or phrases several times because the person you are conversing with does not catch them or understand as fast as they should. Restrain from ridiculing or patronizing the patients about what they say.
Do Not Keep Correcting the Patient
People with dementia do not like it when someone keeps correcting them every time they say something that may not be right. It makes them feel bad about themselves and can make them drift out of the conversation. Discussions should be humorous and light and one should always speak slowly and clearly using simple and short sentences to capture and keep the interest of the dementia patients.
Do Not Get Angry or Upset
When looking after persons with dementia, practicing self-control is of utter importance. Learn how to breathe in and just relax without taking things personally or getting angry and upset. Remember that dementia patients do not act the way they do out of their own accord. It is the illness that makes them behave the way they do.
Do Not Try and Alter Undesirable Behavior
Lack of understanding may push one to try and change or stop any undesirable behavior from patients who have dementia. Keep in mind that it is almost impossible to teach new skills or even reason with the patient. Try instead to decrease frequency or intensity of the behavior. For instance, respond to emotion and not the changes in behavior. If a patient insists on always asking about a particular family member reassure them that he or she is safe and healthy as a way of keeping them calm and happy.
Do Not Try to Stop a Person Who Wants to Leave a Room
Staying in one place for long periods may result in behavior problems in the dementia patient. It is essential to have a safe environment where they can enjoy the outdoors without any problem. When someone tries to leave a room, do not force them to stop. Doing this may result in an extreme reaction such as severe distress or injuries.
Instead, it is best to accompany the patient so that they are safe. You can even suggest going for a drive around the block so that they can experience a new environment for a short period. If they do not want company, just let them go but stay close by to make sure that the patient is safe at all times.
Do Not Expect Too Much
It helps to have an open mind when dealing with an individual who has dementia. Try and keep up with their pace without having to rush them too much. It is advisable to avoid trying to teach new information or ask the affected individuals to do something that they have not previously done.
Do Not Shy Away From Asking For Help
No one may have all the answers especially when it comes to taking care of a person with dementia. Try doing research on how their behavior changes and what needs to be done to help them live their lives without too many complications. Hire help when it becomes too much as it also ensures that you do not become too frustrated or drained. When you have multiple family members who can help, ask everyone to pitch in and look after the patient so that you can get some personal space to breathe and re-energize when it is your time to look after the patient. When you feel like you can no longer look after your loved one at your own home, it may be time to consider assisted living. In such cases, look into dementia care homes that can provide specially trained professionals.
Do Not Panic
When a dementia patient becomes aggressive or agitated, try to remain in control without breaking down, panicking and using physical force. Try other approaches that may help to make them calm. These can include holding their hand firmly but gently, singing them their favorite song, or patting their pack gently. Note that some people do not like to be touched; thus, it is best to give them some space by sitting away from them or leaving the room until they calm down.
Do Not Ignore Physical Abuse
As much as one needs to be tolerant, kind, forgiving, and patient with older adults who have dementia, it does not mean that they have to excuse the patients when they become physically aggressive and allow the abuse to continue. It is not to be accepted, and if it happens, it is best to alert your doctor who will work on the solution to make sure it stops. It will keep both the patient and caregiver in safety.
From physical manifestations to angry outbursts, taking care of an individual with dementia may not be easy. However, working with the tips above can help caregivers and loved ones to get through it. Remember that there are plenty of treatments, interventions and special care providers who can help; therefore, you should never be shy about getting help when you need it.
Infographic: Do’s and Don’ts:
Communicating With a Person Who Has Alzheimer’s Disease
People with Alzheimer’s disease may have trouble finding the right words or remembering what they want to say. This can make communication difficult. Use the tips below to better communicate with a person who has Alzheimer’s.
To share the image, right-click on it and select “save image as” to save the file to your computer. We encourage you to use the hashtag #NIAHealth in your social media posts to connect with people and organizations with similar goals.
“Understanding the infinity of knowledge is the first step in learning to live.”
Kelly Clarkson’s Weight Loss Journey: How She Lost 60 Pounds With Medication, Eating Protein, And Walking
“Everybody thinks it’s Ozempic. It’s not.”
We love that Kelly Clarkson has the voice of an angel, yet she’s still so relatable. Prime example: her journey to get healthier. The Grammy winner recently revealed she’d been ignoring a prediabetes diagnosis for two years before she saw a fateful video of herself. “I was like, ‘Who is that?”” she shared with Whoopi Goldberg on a May 2024 episode of The Kelly Clarkson Show.
While I don’t agree with Whoopi the loudmouth liberal of The View insight into politics. The two discussed what led Kelly to make very down-to-earth changes and drop about 60 pounds. Now, experts say making similar lifestyle tweaks can potentially help millions of us transform our bodies for the better. Keep reading to find out how.
– ALLISON NEMETZ
Discover The Kelly Clarkson Show star’s success secrets-and why experts say they can help the rest of us boost fat burn by up to 900%. The first things most women do to try to get in shape are eating a little better and walking more. Turns out, Kelly really is like us. The number-one strategy she credited with her leaner physique: simply putting one foot in front of the other.
The 42-year old mom, who relocated her show to New York after a messy divorce, began taking her dogs for jaunts in the park, strolling to local shops and restaurants and sauntering through famous museums with daughter River, 10, and son Remy, 8. “Walking in the city is quite the workout,” Kelly explained to People magazine. While she didn’t reveal exactly how much she walks, a New York Times report found people are so likely to walk rather than drive in the Big Apple, the average person logs over 10,000 steps a day-with many getting more than 19,000 steps daily!
Now, walking alone often isn’t enough to move the scale as much as we want it to. For her part, Kelly added other techniques proven to significantly enhance the exercise.
Kelly Clarkson’s 60-Lb. Weight Loss: How Walking Helped Her Slim Down and How You Can, Too
Combining exercise with weight loss meds can supercharge results
After Kelly Clarkson debuted her striking weight loss in 2023, many suspected her success was due to Ozempic. While the Grammy Award-winning musician hasn’t shared which weight loss drug she used, she’s been relatively open about her health journey overall. And it turns out a few simple daily habits—like walking—supercharged her calorie burn and helped her drop weight. Here we break down how walking helped Clarkson lose weight and how you can start reaping the health benefits of regular strolls, too.
Did Kelly Clarkson take Ozempic for weight loss?
While walking did help Clarkson reportedly shed 60 pounds, she also got a boost from using weight loss medication. “I am doing that wonderful shot that works for folks who need some help, and it’s been really good for me,” Clarkson revealed in an episode of The Kelly Clarkson Show last year. “Everyone thinks it’s Ozempic. It’s not,” she clarified, though didn’t share which medication she has taken.
However, she did explain that it helped “break down the sugar—obviously my body doesn’t do it right.”
Ozempic and similar medications (including options like Mounjaro and Zepbound) work by mimicking GLP-1, a hormone that helps control blood sugar and turn off hunger.
Because synthetic GLP-1 doesn’t break down as easily as the real thing, it can “help create the feeling that you just ate dinner, so you don’t want more food,” according to Weill Cornell Medicine obesity expert Louis Aronne, MD, whose most recent research on the drugs appeared in the Journal of the American Medical Association in November 2024.
Kelly says she did not take the type 2 diabetes medication Ozempic for weight loss. During a May episode of The Kelly Clarkson Show, the singer discussed her weight loss with guest Whoopi Goldberg. After Whoopi raved about taking Mounjaro, Kelly opened up about her own experience with taking weight-loss medication.
Kelly shared that she’s lost “a lot” of weight, saying, “Mine is a different one than people assume, but I ended up having to do that too because my bloodwork got so bad.” She added that she did not take Ozempic.
Kelly didn’t name the medication but said that it’s “something that aids in helping break down the sugar—obviously my body doesn’t do it right.”
Kelly said her doctor “chased [her] for, like, two years” to take the medication, but she was nervous of the effects on her thyroid. But ultimately, she decided to take it after she watched a birthday special that she planned to release.“All of a sudden I paused it, and I was like, ‘Who is f*ck is that?’” she said. “You see it and you’re like, ‘Well, she’s about to die of a heart attack,’” Kelly said. Kelly shared that she was 203 pounds at “my heaviest,” but “was never insecure about it.” “I was happy,” she added.
What diagnosis did Kelly Clarkson have?
Kelly had a prediabetes diagnosis, she previously shared on her show.On January 29, Kelly told King of Queens star Kevin James that she “was told I was prediabetic.”“That was literally what happened,” she continued. “They were like — and I was, well, I wasn’t shocked. I was a tiny bit overweight. So, yeah, but I wasn’t shocked by it. But they did. They were like, ‘You’re prediabetic. You’re right on the borderline.’” (Prediabetes means your blood sugar levels are “higher than normal,” but not high enough for a type 2 diabetes diagnosis, per the Centers for Disease Control and Prevention.)
What dress size is Kelly Clarkson?
Kelly hasn’t publicly shared her dress size—and, of course, she doesn’t need to. But an insider told Life & Style that she went from a size 14 to a size 8. “Kelly feels good and is having fun switching up her wardrobe!” the insider added.
How did Kelly Clarkson lose weight?
Kelly’s weight-loss journey was sparked by a cross-country move from Los Angeles to New York. “I was very unhappy in L.A. and had been for several years. I needed a fresh start,” Kelly told People earlier this year. “We told NBC, ‘I’m not trying to sound ungrateful, I just can’t stay here anymore for my mental health; for me and my kids.’ They weren’t doing well either. For the past few years, I’d just been showing up and smiling and doing what I’m supposed to do, but you can only compartmentalize so long until you break.”
But Kelly said that she felt “good” going into season five of her show. “Knowing my kids feel good—and the dust has settled. Season five is my first season to actually enjoy every minute of it.”
This content is imported from poll. You may be able to find the same content in another format, or you may be able to find more information, at their web site.
How many children does Kelly Clarkson have?
Kelly has two children with her ex-husband Brandon Blackstone: Daughter River Rose, 10, and son Remington, 8. Kelly’s kids recently made an appearance on her show, where they seemed super comfortable in front of the camera. Remy even adorably belted out Frank Sinatra’s “My Way” in front of a live studio audience:
“Like their mama, both my kids love singing,” Kelly shared. “And when Remy got to set, he surprised us. He wanted his chance at the microphone, and he literally said, ‘Who do I have to talk to to sing my song?’ I was like, ‘Okay.’ So of course, we made it happen.”
Kelly changed her diet.
Kelly has revamped her diet and is focusing on eating lots of protein. “I eat a healthy mix,” she told People. “I dropped weight because I’ve been listening to my doctor—a couple years I didn’t. And 90 percent of the time I’m really good at it because a protein diet is good for me anyway. I’m a Texas girl, so I like meat—sorry, vegetarians in the world!”
As Kelly noted, her diet is a “healthy mix,” meaning she still allows space for treats.
“I still splurge. The other night I had frozen yogurt with my daughter, and it was magical,” she added.
While on a weight-loss journey in 2018, Kelly said that she would tweak the ingredients in foods to make her meals healthier. “It’s the same stuff you eat—I just use different ingredients,” she said. “Even like fried chicken, I use cassava flour, tapioca, or almond flour, and you use non-hormone chicken.”
But Kelly admitted this isn’t the easiest route to go for most people. “I’m going to be real with you: It’s really expensive to do,” she added.
Kelly later clarified that she’d lost weight following The Plant Paradox by Dr. Steven Gundry. The Plant Paradox Diet is a lectin-free diet that eliminates beans, legumes, whole grains, certain vegetables, and dairy.
“I literally read this book, and I did it for this autoimmune disease that I had and I had a thyroid issue, and now all my levels are back up,” Kelly told Extra that same year. “I’m not on medicine anymore because of this book. It’s basically about how we cook our food, non-GMO, no pesticides, eating really organic…Literally, I haven’t worked out at all!”
Kelly started prioritizing her wellness practices.
In addition to diet and exercise, Kelly shared she’s been indulging in infrared saunas, which have been found to improve sleep, relieve stress and pain, and help clear skin.
She’s also started dabbling in cold plunges. “I just got a cold plunge because everybody wore me down,” Kelly added. Cold plunges are also known to help with cardiovascular health and can boost your metabolism, per Healthline.com.
She keeps a healthy mindset about weight loss.
When Kelly was at her lowest weight in the early 2000s, she was having dark thoughts, per Page Six. “I was miserable, like inside and out, for four years of my life. But no one cared, because aesthetically, you make sense,” she said to Attitude.
“It was a very dark time for me. I thought the only way out was quitting,” she added. “I wrecked my knees and my feet because all I would do is put in headphones and run. I was at the gym all the time.”
Kelly, who has struggled with mental health, has opened up about going to therapy.
“They give you so many tools for how to navigate certain situations and also to have somebody outside your circle that doesn’t know anything, but just knows what’s happening in the now,” she told Entertainment Tonight Canada.
Ultimately, Kelly told People that she’s learned to be kinder to herself, offering this advice to her 15-year-old self: “I’ve always been that kind of person that’s a little hard on oneself. I’d be like, ‘It’s not going to happen anytime soon, but eventually it’ll get easier. Around 41, you’re really going to get your shit together.'”
Kelly hopes to change the way people talk about weight.
Kelly has had to field a lot of talk about her weight over the years. But she told Glamour UK that being thin doesn’t make her feel more confident.
Kelly shared that, at once point in her career, she was asked to have a body like other women in the industry. “It was more of magazines shoved in front of you and, ‘This is what you’re competing with and we’ve got to compete with it,’” she said. “I can’t compete with that. That’s not even my image. That’s not who I am. That’s who they are. We’re all different and it’s okay. I fought more when I was thinner than I do now, because now I just walk in and I just look at them like, ‘I dare you to say something. I’m happy in my life. I’ll work on me in my time!’”
She also pointed out that she got her coaching role on The Voice after she gained weight. “I got on the No. 1 television show at my heaviest point, because it was right after I had kids, and they didn’t care,” she said.
Paul Telegdy, the chairman of NBC Entertainment, hired her “because he loved my personality, he loved that I connect with people and I’m really raw and real,” she said.
“It had nothing to do with my sex appeal or my look aesthetically,” she said. “It had to do with me as a person. I think it’s really up to artists to force people to have that mentality.”
Now, Kelly has gotten rid of the “negative people” in her life, instead embracing the positive ones.
“It was a case of turning around, facing them and walking toward the light,” she told Attitude.
When Kelly began to get noticeably smaller, rumors circulated that she was on weight-loss drugs. She soon confirmed the rumor was true. “Everyone thinks it’s Ozempic-it’s not. It’s something else,” she shared with Whoopi. Kelly added that at first she resisted a prescription: “My doctor chased me for like two years, and I was like, ‘No, I’m afraid of it.’ What changed her mind? “My blood work got so bad,” she said.
Protein is Key Too
Doctors tend to recommend that those of us at risk for diabetes should avoid excess carbohydrates. which can wreak havoc on blood sugar levels. European research shows that those on a protein rich diet that limit starch and sugar experience biochemical shifts that naturally increase GLP-1 production. Plus when you cut back on carbs you begin to turn fat into fuel called ketones. Ketones increase fat burn up to 900% and help destroy appetite. Also pair a low carb diet with walking and you should see awesome results with no prescriptions needed.
Does Kelly use a crazy strict Keto Diet?
Nope. She has shared that her menus are a healthy mix and she aims to make good choices 90% of the time/ So if you want to follow Kelly’s lead, start walking and take other steps to improve your health. But also enjoy every step of the way no matter how far you are from your goal. Because Kelly just doesn’t just walk to get fit, she’s all about walking toward the light to a better life. Another life lesson Kelly learned id that the kinder you are to yourself — getting healthier or anything you want is much easier.
Foods that work like Ozempic
Ozempic, Wegovy and Zepbound quiet “food noise” by increasing levels of the hormone GLP-1. The drugs can be especially helpful for those with type 2 diabetes or who struggle to keep their blood sugar levels in check, like Clarkson.
But if you’d rather try a natural approach, you can mimic the effect of GLP-1 meds with certain foods. A Norwegian study found a low-carb diet keeps GLP-1 high specifically in women—and a free app like Carb Manager can help you hit healthy carb goals for your body. To further enhance the effect, incorporate the following options:
Protein and calcium. Calcium from dairy or greens pairs with amino acids in any protein source to “potently stimulate GLP-1 release,” per a 2021 study in the journal Advanced Nutrition.
Antioxidant bombs. Polyphenol antioxidants in colorful produce, spices, nuts, coffee, tea and cocoa have been shown to seriously spike GLP-1 levels.
Allulose. Zero-cal sweetener allulose (found in trace amounts in figs) is proven to rev GLP-1 and speed weight loss.
How did Kelly Clarkson lose weight?
Before divulging whether she took weight loss injections, The Since U Been Gone singer also revealed that she was prediabetic, something that kick-started her new healthier lifestyle. “I wasn’t shocked,” Clarkson admitted on her talk show. “I was a tiny bit overweight…they were like, ‘You’re prediabetic. You’re right on the borderline.’”
“My heaviest, I was like 203 [pounds], and I’m 5 foot 3 and a half,” she continued. “My doctor chased me for like two years, and I was like, ‘No I’m afraid of it.’” But when her blood work got “so bad”, she changed her mind and reconsidered weight loss drugs.
To help shed unwanted pounds and work toward reversing her prediabetes, Clarkson pointed to infrared saunas, a balanced, protein-centric diet (that includes the occasional sweet treat) and an active lifestyle as the forces behind her progress.
“Walking in the city is quite the workout,” Clarkson told People while discussing how her life has changed since moving to New York City. The Kelly Clarkson Show relocated to NBC Studios in Manhattan in October 2023 after shooting the first four seasons in Los Angeles.
After winning American Idol in 2002, “I wrecked my knees and my feet because all I would do is put in headphones and run. I was at the gym all the time,” Clarkson told the magazine Attitude. Her switch to walking—a low-impact, high-reward form of exercise—is an example of the many ways she’s learned to go easier on her body while still hitting her goals.
Now, when she’s not filming, Clarkson spends her days with her son and daughter, walking all over the big apple, from visiting museums to bringing their dogs to the park, she shared.
And that’s something that has supercharged her results. Both walking and meds work separately, but it’s together that they tend to make magic. In fact, research shows that combining walking, a healthy diet and an Ozempic-style weight-loss med can help people lose up to 22 percent of their body weight.
How walking aids weight loss
Generally speaking, New York City it’s extremely pedestrian-friendly and traveling on foot is part of everyday life for most people.
“Living in a city like NYC incorporates a lot of walking into daily activities, which is great for your overall health,” says Chris Mohr, PhD, RD, fitness and nutrition advisor at Fortune Recommends Health. “All movement counts, and research suggests those who move more regularly are not just fitter, but generally weigh less as well.”
Because walking inherently fits into (and is sometimes even required for) errands, activities, socialization and commuting in the city, it’s an accessible option for most people, he explains.
“Instead of dedicating an hour or two a day to exercise and being sedentary otherwise, walkable cities encourage you to perform what are called exercise snacks: short bouts of activity spread throughout the day,” adds Jake Dickson, CPT-NASM, Certified Personal Trainer at BarBend.
These manageable spurts can serve as building blocks to reach your goal. No matter where you live, Steven Shamah, MD, Chief of Endoscopy at Lenox Hill Hospital in New York, encourages his patients to log at least 10,000 steps a day. Once you start consistently achieving 10,000 steps every day, you can gradually increase it for even more health benefits, if you’re able, he suggests.
“Though walking is not the complete puzzle for weight loss, it is an important one to couple with a healthy diet, quality sleep and stress relief,” Dr. Shamah says.
How to make walking for weight loss easier
While it’s inarguably simpler to get more steps in if you live in a walkable city like Clarkson does, it’s still possible to infuse more walking into your daily life in other creative ways. Here’s how:
One thing that can be helpful is dedicating some time at the start and finish of your day to walk. In the mornings before breakfast and evenings after dinner, walk for 10 to 30 minutes, advises Dickson. These increments will depend on how much free time you have, but they ultimately add up (and can even improve digestion, too, he adds.)
Get more out of short distances
When possible, parking your car farther away than you need to and taking stairs instead of elevators or escalators is also beneficial, experts say. If you use public transportation, have some time to spare and the distance is not too far, see if you can disembark your bus or train one stop early and walk the rest of the way to your destination to burn more calories.
Walk and talk
You can also try swapping in some walking when you’d normally be sitting. Grabbing coffee with a friend? Chat and sip while you stroll. When talking on the phone, stand up and move around during the call.
We know and love how convenient online shopping can be, but when you’re able, opt to go to the store and explore while walking up and down the aisles instead. Work in an office? Take mini breaks to take a lap or two around the building throughout the day. And if you’re logging some time on your computer or watching a TV show at home, invest in a walking pad or treadmill so you can multitask!
Kelly Clarkson clarified that she is not taking Ozempic, which is an FDA-approved prescription medication for people with type 2 diabetes. Although she did not name the specific medication she was prescribed, it was previously revealed that she used Mounjaro, which also treats Type 2 Diabetes. people.com+1
GMOs (genetically modified organisms) are plants, animals, or microorganisms whose DNA has been altered using biotechnology to introduce desirable traits, such as resistance to pests or improved nutritional content. While GMOs have been praised for their potential to increase food security and reduce the need for chemical pesticides, they are also controversial. Critics raise concerns about environmental impact, health risks, and ethical considerations. However, scientific consensus generally supports that GMOs are safe to eat and can offer significant agricultural benefits when properly regulated.
Lip Reader Deciphers Taylor Swift’s Five-Word Response to the Boos ~
Lip reader reveals Taylor Swift’s five-word reaction after getting booed.
It’s sad in our country how Americans focus on the negative and often overlook the good things We The People Do for Others.
Taylor Swift is one of the world’s richest and most powerful women, crossing over into billionaire territory in 2023 thanks to her blockbuster Eras Tour and record-selling Taylor’s Version releases. In fact, Billboardestimated in December 2023 that Swift earned nearly $2 billion that year through her music, tour and accompanying tour film and merch — before even accounting for additional revenue from things such as syncs and sponsorships.
The “Anti-Hero” singer has put her hard-earned wealth to personal use. She’s spent hundreds of millions of dollars on properties in New York City, California, Nashville, Rhode Island and more. She frequently travels via private jet, reportedly owning not just one, but two Dassault Falcon aircrafts. And her much-studied sense of style is aided by pricey, oftentimes designer pieces.
But for those who have crossed her path, Swift has also long been generous with her riches. Through the years, the pop superstar has supported various causes, donated to charities and struggling individuals alike, and showered her fans with lavish presents in a 2014 gift-giving extravaganza known by her fandom as “Swiftmas.”
Swift has been known to be generous with her time.
Whether it’s meeting fans after almost every show of her pre-Eras tours completely free of charge, or making surprise appearances at unsuspecting Swifties’ weddings, bridal showers or engagement parties. There have also been times where fans have opened their front doors to find the musician waiting outside, as well as days spent dropping in to cheer up patients at hospitals. Not to mention, she donated generously to various food banks around the globe where her Eras Tour touched down.
In the fifth and last Super Bowl, the Philadelphia Eagles defeated the Kansas City Chiefs by a score of 40-22, destroying any possibility of the Chiefs creating history.
In spite of the fact that the Chiefs were attempting to make history by becoming the first team to win a championship three times in a row, they struggled throughout the game, with Travis Kelce having a particularly quiet night.
While attending the event to show her support for her boyfriend Kelce, pop icon Taylor Swift found herself at the focus of unanticipated reaction. This added to the tension that was already present.
Taylor Alison Swift was born on December 13, 1989, in West Reading, Pennsylvania.[1] She is named after the singer-songwriter James Taylor.[2][3] Her father, Scott Kingsley Swift, was a stockbroker for Merrill Lynch, and her mother, Andrea Gardner Swift (née Finlay), worked as a mutual fund marketing executive.[4] Swift’s younger brother, Austin, is an actor.[5] Their maternal grandmother, Marjorie Finlay (née Moehlenkamp), was an opera singer,[6] whose singing in church became one of Swift’s earliest memories of music that shaped her career.[4] Swift is of Scottish, English, and German descent, with distant Italian and Irish ancestry.[7][8][9]
Swift spent her early years on a Christmas tree farm in Pennsylvania that her father had purchased from one of his clients,[10] and she spent her summers at her family’s vacation home in Stone Harbor, New Jersey, where she occasionally performed acoustic songs at a local coffee shop.[11]
At 11, Swift traveled to Nashville with her mother to visit record labels and submit demo tapes of Dolly Parton and Dixie Chicks karaoke covers.[22] She was rejected by all the labels, which led her to focus on songwriting.[23] She started learning the guitar at 12 with the help of Ronnie Cremer, a computer repairman and local musician who also assisted Swift with writing an original song.[24]
Matthew 7:7 “Continue to ask, and God will give it to you. Continue to search, and you will find. Continue to knock, and the door will open for you.”
In 2003, Swift and her parents started working with the talent manager Dan Dymtrow. With his help, Swift modeled for Abercrombie & Fitch and had an original song included on a Maybelline compilation CD.[25] After performing original songs at an RCA Records showcase, 13-year-old Swift was given an artist development deal and began to travel regularly to Nashville with her mother.[26][27]
To help Swift break into the country music scene, her father transferred to Merrill Lynch’s Nashville office when she was 14 years old, and the family relocated to Hendersonville, Tennessee.[28][29]
Taylor Swift – Wikipedia, had previously demonstrated her enthusiasm for the Eagles. In fact, she was even seen wearing a Philadelphia Eagles hoodie while she was out and about in New York City.
On the other hand, when she started dating Kelce, her loyalty gravitated toward the Chiefs out of natural instinct. She has been a regular at Chiefs games ever since their connection became public knowledge, and she has been seen applauding from the fans when they play.
In spite of her unflinching backing, the crowd in New Orleans did not demonstrate the same level of warmth. An audience that was cheering for the Eagles erupted in loud boos when the cameras in the stadium panned to Taylor Swift.
The scene was instantly picked up by social media, and admirers began to speculate about her reaction to the situation there. Swift reportedly turned to others surrounding her and asked, “Aww what, what’s going on?” With a genuine expression of surprise on her face, as reported by multiple media outlets.
The occurrence generated debate almost immediately.
There were others who believed that the boos were due to her shift in her allegiance to the squad, while others, including the former President Donald Trump, took a different approach.
In an article that he published on Truth Social.
Trump asserted that the reaction was spurred by his followers. He wrote, “The only one that had a tougher night than the Kansas City Chiefs was Taylor Swift.” As she was leaving the stadium, she was booed. It is really difficult to forgive MAGA!
Those who disagreed with this viewpoint were not unanimous. Serena Williams, a tennis legend, rushed to Swift’s rescue and posted on X, “I love you @taylorswift13 don’t listen to those booo!!” Swift immediately responded to Williams’s tweet.
In the meantime, numerous rumors circulated prior to the game on whether or not Kelce would make a marriage proposal to Swift in the event that the Chiefs achieved a historic victory. By contrast, Kelce was observed leaving the arena by himself, while Swift was nowhere to be found as the night came to a disappointing conclusion for Kansas City.